Tang Vivi, Wieslander Elinore, Haghanegi Mahnaz, Kjellén Elisabeth, Alkner Sara
Skåne University Hospital, Department of Hematology, Oncology and Radiation Physics, 222 42 Lund, Sweden.
Lund University, Faculty of Medicine, Institute of Clinical Sciences, Department of Oncology, Barngatan 4, 22242 Lund, Sweden.
Clin Transl Radiat Oncol. 2025 May 28;53:100986. doi: 10.1016/j.ctro.2025.100986. eCollection 2025 Jul.
Target volume delineation is crucial in breast cancer radiotherapy planning but involves significant interobserver variability. Deep learning (DL) models may reduce this variability, saving time and costs. However, current DL-models do not consider clinical data, such as tumor location and patient comorbidity, to adjust the target and reduce dose to organs at risk (OAR). This study compares clinically defined target volumes to those generated by a DL-model in terms of size, geometric overlap, and dose to OAR.
For a hypothetical breast cancer patient, we compared target volumes constructed by Swedish radiotherapy clinics and two DL-models, Raystation and MVision. Geometrical overlap was evaluated, as well as the impact of differences in target delineation on dose to OAR. Treatment plans for locoregional vs. breast-only 3D-conformal radiotherapy were generated.
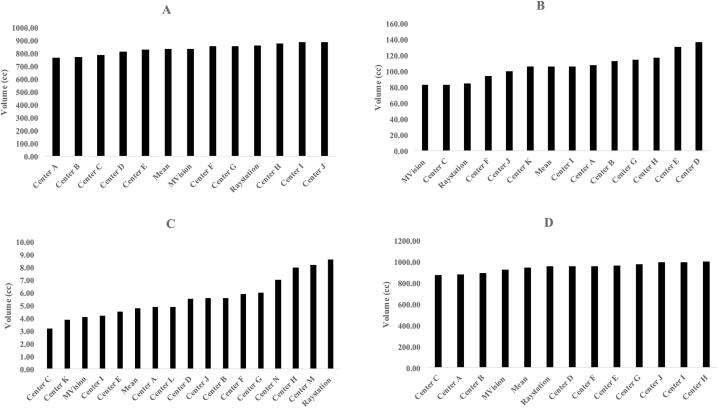
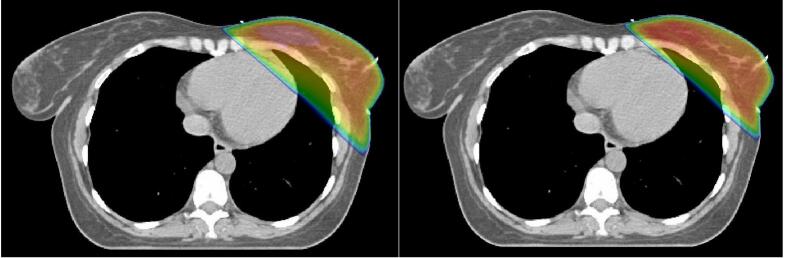
CTV-structures for the breast, lymph nodes level I-IV, and internal mammary nodes were available for 10, 11, and 14 centers respectively. Volume of the CTV-breasts varied between 770-890cc, and the total CTV-volumes (breast + lymph nodes) between 875-1003cc. The DL-models did not constitute the largest nor smallest breast or total CTV-volumes, and geometric overlap between structures was relatively good. Evaluating dose to OAR from dose plans based on the respective CTV-volumes for locoregional radiotherapy, this was comparable between the DL-models and the mean of the CTVs generated by the clinics. In radiotherapy of only the breast, the CTV-breasts constructed by the DL-models gave the highest heart doses due to their proximity to the chest wall, affecting field angle choices. No difference was seen in dose to the ipsilateral lung, thyroid gland, or humeral head.
DL-models for target delineation have great potential. However, their introduction must be closely monitored since even small differences compared to clinical standards may affect doses to OAR in 3D conformal breast cancer radiotherapy.
靶区勾画在乳腺癌放疗计划中至关重要,但存在显著的观察者间差异。深度学习(DL)模型可能会减少这种差异,节省时间和成本。然而,当前的DL模型并未考虑临床数据,如肿瘤位置和患者合并症,以调整靶区并减少危及器官(OAR)的剂量。本研究在大小、几何重叠以及对OAR的剂量方面,比较了临床定义的靶区体积与DL模型生成的靶区体积。
对于一名假设的乳腺癌患者,我们比较了瑞典放疗诊所构建的靶区体积以及两个DL模型(Raystation和MVision)生成的靶区体积。评估了几何重叠以及靶区勾画差异对OAR剂量的影响。生成了局部区域放疗与仅乳房3D适形放疗的治疗计划。
分别有10个、11个和14个中心提供了乳房、Ⅰ-Ⅳ级淋巴结和内乳淋巴结的临床靶体积(CTV)结构。CTV乳房的体积在770 - 890立方厘米之间,CTV总体积(乳房 + 淋巴结)在875 - 1003立方厘米之间。DL模型生成的乳房或CTV总体积既不是最大的也不是最小的,结构之间的几何重叠相对较好。基于局部区域放疗各自的CTV体积评估剂量计划对OAR的剂量,DL模型与诊所生成的CTV平均值之间具有可比性。在仅乳房放疗中,DL模型构建的CTV乳房由于靠近胸壁,导致心脏剂量最高,影响了射野角度的选择。同侧肺、甲状腺或肱骨头的剂量没有差异。
用于靶区勾画的DL模型具有巨大潜力。然而,必须密切监测其引入情况,因为与临床标准相比即使是微小差异也可能影响3D适形乳腺癌放疗中对OAR的剂量。