Zhang Teng, Li Jian, Li Xinyu, Pan Xin, Gao Xianlei, Yang Xiaojie, Ma Xiaolin, Li Hao, Feng Shiqing, Liu Zhongjun
Department of Orthopedics, Qilu Hospital of Shandong University, Shandong University, Jinan, 250012, China.
Beijing AK Medical Co., Ltd., China.
J Orthop Translat. 2025 Jun 5;53:52-62. doi: 10.1016/j.jot.2025.04.010. eCollection 2025 Jul.
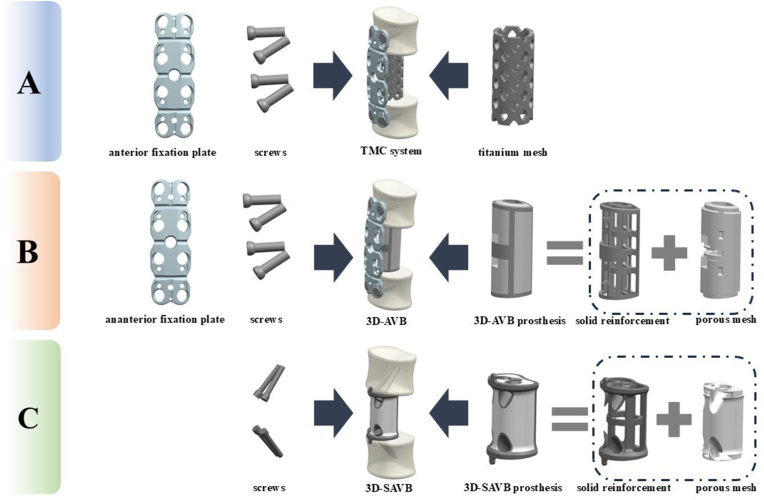
Corpectomy and bone defects reconstruction is a key surgical technique in spinal diseases treatment. Popular bone defect reconstruction methods include titanium mesh cage (TMC) fixation plate systems and traditional 3D-printed artificial vertebral body (3D-AVB). In our previous study, we conceptualised and created a self-stabilised 3D-printed artificial vertebral body (3D-SAVB) system and tested its clinical safety and efficacy, but have not compared with the conventional implants. This study was designed to compare our innovative 3D-SAVB system with a conventional 3D-AVB system, both mechanically and clinically.
This study included 33 patients with cervical spondylotic myelopathy who underwent single-level ACCF using the TMC, 3D-AVB, and 3D-SAVB systems. The operation time, intraoperative blood loss, neurological function recovery rate, average subsidence length, and cervical lordosis correction (C2-7 Cobb angle change) rates of the TMC, 3D-AVB, and 3D-SAVB groups were tested to compare their performance, and we selected four representative clinical cases with various diseases who underwent 3D-SAVB surgery for follow-up studies to demonstrate the clinical effect. In addition, finite element analysis was used to compare the stability, stress distribution, and artificial vertebral body stress of the 3D-SAVB, 3D-AVB, and TMC systems.
The neurological function recovery rates of the TMC (84.8 ± 10.7 %), 3D-AVB (74.3 ± 7.9 %), and SAVB (85.99 ± 13.2 %) groups showed no significant difference (p > 0.05). The mean operation time of the TMC group (119.3 ± 21.5 min) is significant more than the 3D-SAVB (76.1 ± 23.1 mm) and 3D-AVB (82.6 ± 21.3 mm) groups (p < 0.05). The intraoperative blood loss of the TMC group (218.2 ± 51.5 ml) was significantly greater than that of the 3D-SAVB (187.6 ± 43.2 ml) and 3D-AVB groups (195.6 ± 31.3 ml) (p < 0.05). The mean subsidence length of the TMC group (3.5 ± 0.6 mm) was significantly greater than the 3D-AVB (1.3 ± 0.5 mm, p < 0.001) and 3D-SAVB (1.2 ± 1.1 mm, p = 0.002). The lordosis correction (C2-7 Cobb angle change) rate of the 3D-SAVB [(60.38 ± 6.2)%] and 3D-AVB [(61.4 ± 7.9)%] groups was significantly higher than that of the TMC group [(32.35 ± 3.7)%] (p < 0.05). Patients treated with the 3D-SAVB system achieved satisfactory treatment results with no postoperative complications during the follow-up period. The failed TMC fixation plate system underwent revision surgery using 3D-SAVB and demonstrated a superior prognosis. The biomechanical test showed that the 3D-SAVB system had greater longitudinal stability (p < 0.01), better stress distribution (p < 0.01), and less vertebral stress (p < 0.01) than the 3D-AVB and TMC systems.
These results demonstrate the mechanical advantages and great clinical application potential of our innovative 3D-SAVB system for challenging spinal surgeries.
The 3D-SAVB system eliminates the need for supplementary fixation plates, reduces surgical complications like subsidence, and improves cervical lordosis correction. Its biomechanical superiority and clinical efficacy support its adoption as a next-generation spinal implant.
椎体切除及骨缺损重建是脊柱疾病治疗中的一项关键手术技术。常用的骨缺损重建方法包括钛网笼(TMC)固定板系统和传统的3D打印人工椎体(3D - AVB)。在我们之前的研究中,我们构思并创建了一种自稳定3D打印人工椎体(3D - SAVB)系统,并测试了其临床安全性和有效性,但尚未与传统植入物进行比较。本研究旨在从力学和临床方面将我们创新的3D - SAVB系统与传统的3D - AVB系统进行比较。
本研究纳入了33例脊髓型颈椎病患者,他们分别接受了使用TMC、3D - AVB和3D - SAVB系统的单节段ACCF手术。测试了TMC、3D - AVB和3D - SAVB组的手术时间、术中出血量、神经功能恢复率、平均下沉长度以及颈椎前凸矫正(C2 - 7 Cobb角变化)率,以比较它们的性能,并且我们选择了4例患有各种疾病并接受3D - SAVB手术的具有代表性的临床病例进行随访研究,以证明临床效果。此外,使用有限元分析来比较3D - SAVB、3D - AVB和TMC系统的稳定性、应力分布和人工椎体应力。
TMC组(84.8 ± 10.7%)、3D - AVB组(74.3 ± 7.9%)和SAVB组(85.99 ± 13.2%)的神经功能恢复率无显著差异(p > 0.05)。TMC组的平均手术时间(119.3 ± 21.5分钟)显著长于3D - SAVB组(76.1 ± 23.1毫米)和3D - AVB组(82.6 ± 21.3毫米)(p < 0.05)。TMC组的术中出血量(218.2 ± 51.5毫升)显著大于3D - SAVB组(187.6 ± 43.2毫升)和3D - AVB组(195.6 ± 31.3毫升)(p < 0.05)。TMC组的平均下沉长度(3.5 ± 0.6毫米)显著大于3D - AVB组(1.3 ± 0.5毫米,p < 0.001)和3D - SAVB组(1.2 ± 1.1毫米,p = 0.002)。3D - SAVB组[(60.38 ± 6.2)%]和3D - AVB组[(61.4 ± 7.9)%]的前凸矫正(C2 - 7 Cobb角变化)率显著高于TMC组[(32.35 ± 3.7)%](p < 0.05)。接受3D - SAVB系统治疗的患者在随访期间取得了满意的治疗效果,且无术后并发症。失败的TMC固定板系统使用3D - SAVB进行了翻修手术,预后良好。生物力学测试表明,3D - SAVB系统比3D - AVB和TMC系统具有更大的纵向稳定性(p < 0.01)、更好的应力分布(p < 0.01)和更小的椎体应力(p < 0.01)。
这些结果证明了我们创新的3D - SAVB系统在具有挑战性的脊柱手术中的力学优势和巨大的临床应用潜力。
3D - SAVB系统无需辅助固定板,减少了下沉等手术并发症,并改善了颈椎前凸矫正。其生物力学优势和临床疗效支持其作为下一代脊柱植入物被采用。