Xie Shuqi, Zhao Xi, Zhao Zitong, Gui Min, Cao Xiaodan, Shen Xiyuan, Luo Junjie, Chen Xiaorui, Xia Yuxuan, Yu Bin
Department of Anesthesiology, Tongji Hospital, School of Medicine, Tongji University, Shanghai, People's Republic of China.
Department of Anesthesiology and Pain Rehabilitation, Shanghai YangZhi Rehabilitation Hospital, School of Medicine, Tongji University, Shanghai, People's Republic of China.
J Pain Res. 2025 Jun 12;18:2947-2960. doi: 10.2147/JPR.S523812. eCollection 2025.
Delayed neurocognitive recovery is common in elderly patients undergoing major surgery under general anesthesia. We conducted a randomized controlled trial to examine whether continuous femoral nerve block plus sacral plexus block reduces the rate of delayed neurocognitive recovery in patients undergoing hip surgery.
This is a single-centre, randomized controlled trial. Patients undergoing hip surgery were randomized (1:1 ratio) to undergo surgery under either continuous femoral nerve block plus sacral plexus block or general anesthesia. The primary end point was delayed neurocognitive recovery, as assessed using a battery of neuropsychological tests at 7 days after the surgery ( score ≤-1.96 in at least 2 tests, and/or combined score ≤-1.96), in a modified intent-to-treat population. Secondary end points included postoperative complications, moderate/severe postoperative pain (visual analogue scale ≥4), use of opioids within 48 hours, and 6-month all-cause mortality.
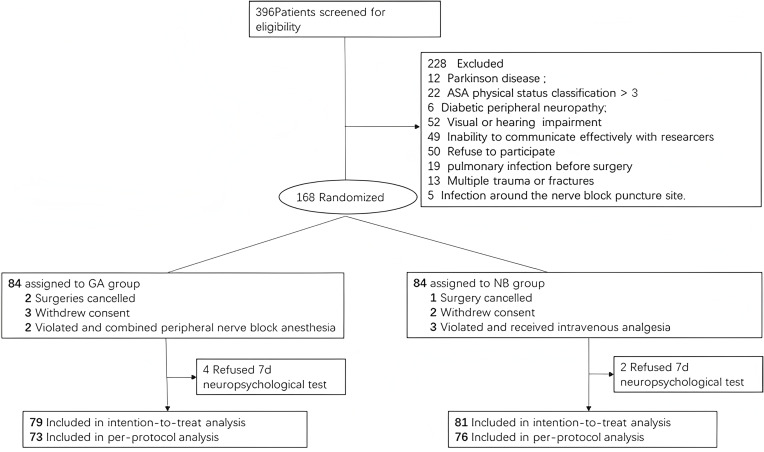
A total of 168 patients were enrolled from January 2018 to May 2021. One hundred and sixty were included in the analysis (81 and 79 in the nerve block and general anesthesia, respectively). The rate of delayed neurocognitive recovery was 7.4% (6/81) in the continuous femoral nerve block plus sacral plexus block group versus 21.5% (17/79) in the general anesthesia group (odds ratio: 0.34, 95% CI: 0.14-0.83; P = 0.01). The rate of postoperative pulmonary infection was 1.2% (1/81) in the nerve block group versus 10.1% (8/79) in the general anesthesia group OR 0.12 (95% CI 0.02,0.95; P = 0. 02). No patient died within 6 months after surgery.
When compared with general anesthesia, continuous nerve block anesthesia might decrease the incidence of delayed neurocognitive recover in patients undergoing hip fracture surgery. The locoregional anesthesia technique for patients undergoing hip surgery offers a safer alternative that lowers the risk of complications.
在接受全身麻醉的大手术老年患者中,延迟性神经认知功能恢复很常见。我们进行了一项随机对照试验,以研究连续股神经阻滞联合骶丛阻滞是否能降低髋关节手术患者延迟性神经认知功能恢复的发生率。
这是一项单中心随机对照试验。接受髋关节手术的患者按1:1比例随机分为两组,分别接受连续股神经阻滞联合骶丛阻滞或全身麻醉下的手术。主要终点是延迟性神经认知功能恢复,在改良意向性分析人群中,于术后7天使用一系列神经心理学测试进行评估(至少2项测试得分≤ -1.96,和/或综合得分≤ -1.96)。次要终点包括术后并发症、中度/重度术后疼痛(视觉模拟评分≥4)、48小时内使用阿片类药物情况以及6个月全因死亡率。
2018年1月至2021年5月共纳入168例患者。160例纳入分析(神经阻滞组81例,全身麻醉组79例)。连续股神经阻滞联合骶丛阻滞组延迟性神经认知功能恢复发生率为7.4%(6/81),全身麻醉组为21.5%(17/79)(优势比:0.34,95%可信区间:0.14 - 0.83;P = 0.01)。神经阻滞组术后肺部感染发生率为1.2%(1/81),全身麻醉组为10.1%(8/79),优势比为0.12(95%可信区间0.02,0.95;P = 0.02)。术后6个月内无患者死亡。
与全身麻醉相比,连续神经阻滞麻醉可能降低髋关节骨折手术患者延迟性神经认知功能恢复的发生率。髋关节手术患者采用局部区域麻醉技术提供了一种更安全的选择,可降低并发症风险。