Beyer Rebecca Elisabeth, Müller Maximilian Leo, Doeblin Patrick, Werhahn Stefanie Maria, Chiribiri Amedeo, Tschöpe Carsten, Sampath Smita, Atkins G Brandon, Cislak Dawn, Bautmans An, Palcza John, McAvoy Tom, Bakar Asad Abu, Lee Anita Y H, Zhao Xuemei, Posch Maximilian G, Wieditz Johannes, Tanacli Radu, Zieschang Victoria, Nassar Mithal, Zamani Seyedeh Mahsa, Stehning Christian, Edelmann Frank, Hashemi Djawid, Kelle Sebastian
Department of Cardiology, Angiology and Intensive Care Medicine, Deutsches Herzzentrum der Charité- Medical Heart Center of Charité and German Heart Institute Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353, Berlin, Germany.
Charité- Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität Zu Berlin, Charitéplatz 1, 10117, Berlin, Germany.
Cardiovasc Diabetol. 2025 Jun 18;24(1):258. doi: 10.1186/s12933-025-02808-3.
The diagnostic criteria for HFpEF remain inconsistently defined, further confounded by comorbidities such as obesity and type 2 diabetes mellitus (T2DM), which are thought to contribute to its pathogenesis via chronic pro-inflammatory mechanisms. This study aimed to evaluate the relationship between advanced cardiac magnetic resonance (CMR) imaging and pro-fibrotic and inflammatory serum biomarkers, assessing their potential to discriminate HFpEF from associated comorbid conditions.
This was an exploratory analysis of a prospective cohort study of 35 obese/overweight participants (mean age 64 ± 8 years, 23% females), including 16 with T2DM, 13 with HFpEF (NYHA II-III) and T2DM, and 6 healthy controls. All subjects underwent comprehensive contrast-enhanced CMR at a 3 T scanner (Philips Ingenia, The Netherlands), including assessment of left ventricular and left atrial (LA) volumetry and function, myocardial perfusion reserve (MPR), and diffuse fibrosis imaging (ECV). Obtained serum biomarkers were Pentraxin-3, Galectin-3 and Interleukin-1 Receptor-Like 1 (IL1RL1). Statistical analyses included one-way ANOVA, Tukey test, Pearson's correlation, regression and receiver operating characteristic analyses, and intra-class correlation.
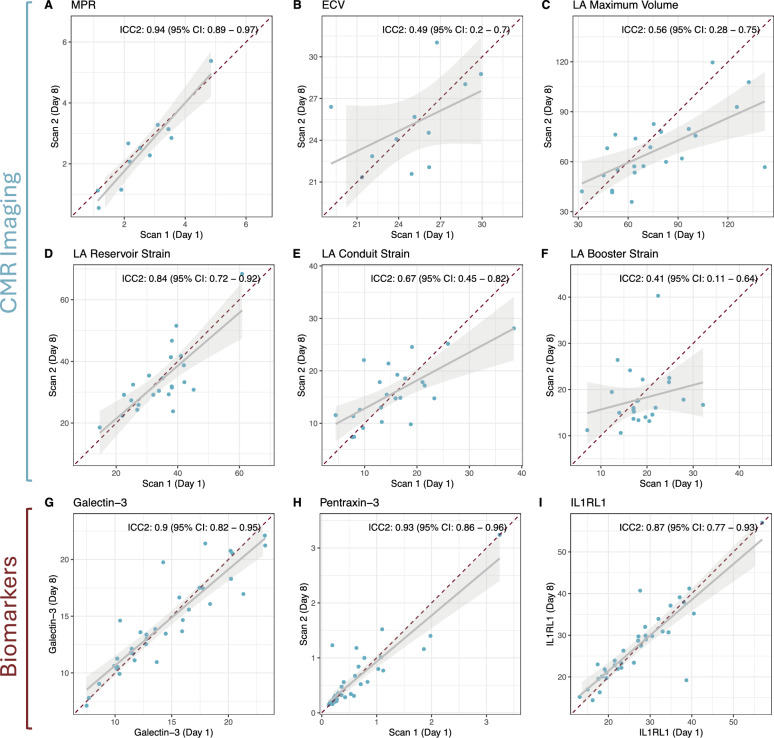
In multivariable regression, impaired measures of LA structure and function emerged as the only independent discriminators of HFpEF, with LA maximum volume showing an OR of 1.13 (95% CI 1.05-1.28), reservoir strain of 0.71 (95% CI 0.44-0.89), conduit strain of 0.57 (95% CI 0.32-0.82) and booster strain of 0.70 (95% CI 0.48-0.89) per unit increase. No differences in MPR nor ECV were observed between the groups. While serum biomarkers Galectin-3 and Pentraxin-3 were significantly higher in HFpEF vs. obese controls (16.1 ng/ml ± 3.8 ng/ml vs. 10.6 ng/ml ± 3.7 ng/ml, p = 0.011, and 0.84 ng/ml ± 0.67 ng/ml vs. 0.21 ng/ml ± 0.05 ng/ml, p = 0.031, respectively), these biomarkers remained within normal limits and showed only moderate correlations with CMR metrics. Highest inter-study reproducibility was seen in MPR (ICC: 0.94), LA Reservoir Strain (ICC: 0.84) and serum biomarkers (ICC: 0.087-0.93).
CMR markers of diffuse fibrosis and microvascular dysfunction may not differentiate HFpEF from obese or diabetic controls. However, left atrial function assessment may evolve to be a reproducible and practical CMR marker, effectively distinguishing HFpEF independent of fibrotic remodeling.
射血分数保留的心力衰竭(HFpEF)的诊断标准仍未统一界定,肥胖和2型糖尿病(T2DM)等合并症使其更加复杂,这些合并症被认为通过慢性促炎机制参与其发病过程。本研究旨在评估心脏磁共振成像(CMR)与促纤维化和炎症血清生物标志物之间的关系,评估它们区分HFpEF与相关合并症的潜力。
这是一项对35名肥胖/超重参与者(平均年龄64±8岁,23%为女性)的前瞻性队列研究的探索性分析,其中包括16名T2DM患者、13名HFpEF(纽约心脏协会II-III级)合并T2DM患者和6名健康对照者。所有受试者均在3T扫描仪(荷兰飞利浦Ingenia)上接受了全面的对比增强CMR检查,包括评估左心室和左心房(LA)容积及功能、心肌灌注储备(MPR)和弥漫性纤维化成像(ECV)。检测的血清生物标志物有3型 pentraxin、半乳糖凝集素-3和白细胞介素-1受体样1(IL1RL1)。统计分析包括单因素方差分析、Tukey检验、Pearson相关性分析、回归分析和受试者工作特征分析以及组内相关性分析。
在多变量回归分析中,LA结构和功能受损指标是HFpEF的唯一独立鉴别因素,LA最大容积每增加一个单位,其比值比为1.13(95%可信区间1.05-1.28),储备应变比值比为0.71(95%可信区间0.44-0.89),管道应变比值比为0.57(95%可信区间0.32-0.82),增强应变比值比为0.70(95%可信区间0.48-0.89)。各组间MPR和ECV无差异。虽然HFpEF组的血清生物标志物半乳糖凝集素-3和3型pentraxin显著高于肥胖对照组(分别为16.1 ng/ml±3.8 ng/ml对10.6 ng/ml±3.7 ng/ml,p=0.011;0.84 ng/ml±0.67 ng/ml对0.21 ng/ml±0.05 ng/ml,p=0.031),但这些生物标志物仍在正常范围内,且与CMR指标仅呈中度相关。MPR(组内相关系数:0.94)、LA储备应变(组内相关系数:0.84)和血清生物标志物(组内相关系数:0.087-0.93)的研究间再现性最高。
弥漫性纤维化和微血管功能障碍的CMR标志物可能无法区分HFpEF与肥胖或糖尿病对照组。然而,左心房功能评估可能会成为一种可重复且实用的CMR标志物,能有效独立于纤维化重塑来鉴别HFpEF。