Oren Daniel, Ramchandani Sunil, Lorenzana Adrian, Nair Ranjit, Szinte Julia, Maalizadeh Kian, Ftiha Farage, Moeller Cathrine M, Fernandez-Valledor Andrea, Cohen Roi Bar, Zepeda Ignacio, Alishetti Shudhanshu, Mihatov Nino, Ramasubbu Kumudha, Minkin Ruth, Saleh Anthony, Parikh Manish A, Fenton Franklyn, Peterson Stephen J
Department of Medicine, New York Presbyterian, Brooklyn Methodist Hospital, Weill Cornell Medicine, NY, USA.
Department of Medicine, Icahn School of Medicine at Mount Sinai West and St. Luke's Hospitals, NY, USA.
Int J Cardiol Heart Vasc. 2025 Jun 7;59:101716. doi: 10.1016/j.ijcha.2025.101716. eCollection 2025 Aug.
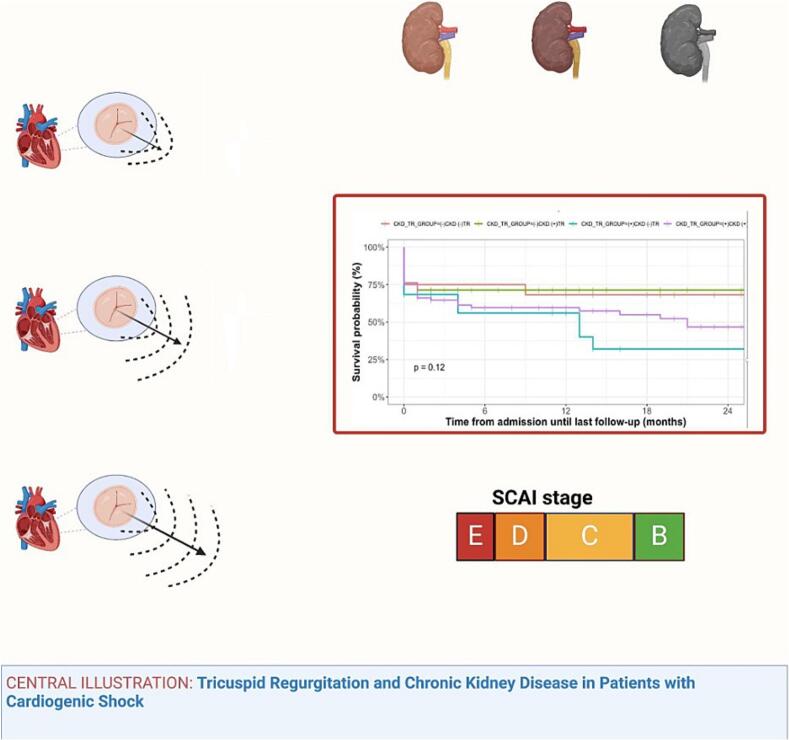
Chronic kidney disease (CKD) frequently complicates Congestive Heart Failure (CHF) and can worsen outcomes in cardiogenic shock. Tricuspid Regurgitation (TR), by elevating central venous pressure, may exacerbate renal impairment. Limited data exist regarding CKD's influence in TR interventions. This study assesses the impact of CKD on survival and explores RV dysfunction as a potential mediator in patients with TR in cardiogenic shock.
We retrospectively analyzed patients admitted with HF-related or myocardial infarction-induced cardiogenic shock (2021-2025). Patients were stratified by TR severity (none/trivial, mild, moderate, severe) and CKD stage. Echocardiographic, laboratory, and hemodynamic data were collected. RV dysfunction was assessed using echocardiography and right heart catheterization. Survival outcomes, including HF readmissions and mortality, were evaluated using Kaplan-Meier analysis and Cox regression, considering predictors significant at p < 0.10.
Among 177 patients (median age 70 years, EF 35 %, 46 % Black), 55 % had CKD. TR severity distribution was: none/trivial 42 %, mild 16 %, moderate 22 %, and severe 20 %. Severe TR significantly increased in-hospital mortality (40 %) compared to non-severe TR (24 %) and correlated with worsening CKD stages. HF readmissions within 12 months occurred in 10 % of patients. Older age and RV dysfunction emerged as the strongest mortality predictors. Severe TR independently increased mortality and readmission risk.
Severe TR significantly worsens survival in cardiogenic shock patients, especially those with advanced CKD, mediated by RV dysfunction. CKD severity assessment may enhance patient stratification for valve interventions. Randomized studies are required to further validate these findings.
慢性肾脏病(CKD)常使充血性心力衰竭(CHF)复杂化,并可能使心源性休克的预后恶化。三尖瓣反流(TR)通过升高中心静脉压,可能会加重肾功能损害。关于CKD对TR干预影响的数据有限。本研究评估CKD对生存率的影响,并探讨右心室功能障碍作为心源性休克TR患者潜在中介因素的作用。
我们回顾性分析了因心力衰竭相关或心肌梗死诱发的心源性休克入院的患者(2021 - 2025年)。患者按TR严重程度(无/轻微、轻度、中度、重度)和CKD分期进行分层。收集了超声心动图、实验室和血流动力学数据。使用超声心动图和右心导管检查评估右心室功能障碍。使用Kaplan - Meier分析和Cox回归评估生存结局,包括心力衰竭再入院率和死亡率,考虑p < 0.10时具有显著意义的预测因素。
在177例患者(中位年龄70岁,射血分数35%,46%为黑人)中,55%患有CKD。TR严重程度分布为:无/轻微42%,轻度16%,中度22%,重度20%。与非重度TR(24%)相比,重度TR显著增加了住院死亡率(40%),并与CKD分期恶化相关。10%的患者在12个月内发生心力衰竭再入院。年龄较大和右心室功能障碍是最强的死亡预测因素。重度TR独立增加死亡率和再入院风险。
重度TR显著恶化心源性休克患者的生存,尤其是那些患有晚期CKD的患者,由右心室功能障碍介导。CKD严重程度评估可能会增强瓣膜干预的患者分层。需要进行随机研究以进一步验证这些发现。