Orazem Miha, Velenik Vaneja, Ihan Alojz
1Division of Radiotherapy, Institute of Oncology Ljubljana, Ljubljana, Slovenia.
2Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia.
Radiol Oncol. 2025 Jun 16;59(2):252-256. doi: 10.2478/raon-2025-0034. eCollection 2025 Jun 1.
Radiation-induced lymphopenia (RIL) is associated with an increased risk of death in solid tumors, including rectal cancer. The aim of this study was to determine whether the sequencing of chemotherapy in total neoadjuvant treatment (TNT) for rectal cancer predicts the development of RIL.
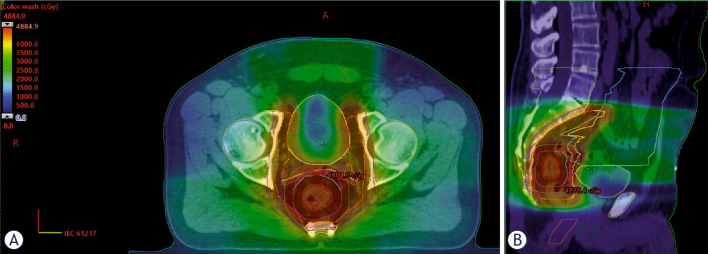
We analyzed acute hematologic toxicity data from 53 patients who underwent TNT for locally or locoregionally advanced rectal cancer between July 2022 and April 2023. Twenty-eight patients received induction chemotherapy with capecitabine and oxaliplatin [CAPOX], and 25 received consolidation chemotherapy (6 cycles of CAPOX in both groups). The chemoradiation protocol consisted of Volumetric Modulated Arc Therapy with Simultaneous Integrated Boost Radiotherapy (VMAT-SIB RT) up to 48.4 Gy in 22 fractions, concomitantly with capecitabine twice a day (, BID). The Mann-Whitney U test was performed to compare RIL between the two patient groups. Pelvic bone marrow was contoured as a non-limiting organ-at-risk to assess the received dose, and binary logistic regression was used to determine whether RIL depends on V~V or the planning target volume (PTV) size.
Thirty-four patients (64.2%) developed RIL of any grade, which was not significantly associated with either the induction or consolidation chemotherapy TNT regimen (Wald = 3.159, p = 0.076). No significant differences were found in neutrophil counts or the neutrophil-to-lymphocyte ratio. In the logistic regression model predicting the likelihood of RIL, two variables were statistically significant: V (Wald = 4.366, p = 0.037) and V (Wald = 6.084, p = 0.014). These results indicate that V< 71% and V< 26.6% may reduce the likelihood of developing RIL.
In our study, the sequencing of chemotherapy in TNT for rectal cancer did not predict the development of RIL. However, the incidence of RIL may be reduced by applying RT dosimetric constraints to the pelvic bone marrow.
放射性淋巴细胞减少(RIL)与实体瘤(包括直肠癌)的死亡风险增加相关。本研究的目的是确定直肠癌全新辅助治疗(TNT)中化疗的顺序是否能预测RIL的发生。
我们分析了2022年7月至2023年4月期间53例接受TNT治疗局部或局部区域晚期直肠癌患者的急性血液学毒性数据。28例患者接受了卡培他滨和奥沙利铂诱导化疗[CAPOX],25例接受巩固化疗(两组均为6周期CAPOX)。放化疗方案包括容积调强弧形放疗联合同步整合加量放疗(VMAT-SIB RT),总剂量达48.4 Gy,分22次,同时卡培他滨每日两次(,每日两次)。采用Mann-Whitney U检验比较两组患者的RIL情况。将盆腔骨髓勾画为非限制性危及器官以评估所接受的剂量,并使用二元逻辑回归确定RIL是否取决于V~V或计划靶体积(PTV)大小。
34例患者(64.2%)发生了任何级别的RIL,这与诱导或巩固化疗TNT方案均无显著相关性(Wald = 3.159,p = 0.076)。中性粒细胞计数或中性粒细胞与淋巴细胞比值无显著差异。在预测RIL可能性的逻辑回归模型中,有两个变量具有统计学意义:V(Wald = 4.366,p = 0.037)和V(Wald = 6.084,p = 0.014)。这些结果表明,V<71%和V<26.6%可能会降低发生RIL的可能性。
在我们的研究中,直肠癌TNT中化疗的顺序不能预测RIL的发生。然而,通过对盆腔骨髓应用放疗剂量学限制,RIL的发生率可能会降低。