Perlow Haley K, Khullar Karishma, Kumar Ritesh, Sasmal Sonya, Nakamoto Kent, Gokun Yevgeniya, Eckstein Jacob, Young Rebekah, Diaz Dayssy A, Martin Douglas, Collier Katharine A, Meng Lingbin, Parikh Rahul R, Clinton Steven, Wang Shang-Jui
Department of Radiation Oncology, The Ohio State University College of Medicine and Comprehensive Cancer Center, 460 W. 10th Avenue, Columbus, OH 43210, USA.
Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, OH 44106, USA.
Curr Oncol. 2025 Jun 15;32(6):353. doi: 10.3390/curroncol32060353.
The treatment efficacy of prostate cancer (PCa) radiotherapy (RT) can be inadvertently affected by the concurrent usage of non-oncologic medications. Many studies have associated the intake of several non-oncologic drugs with cancer specific outcomes. In this study, we report the impact of daily non-oncologic medications including aspirin, metformin, and statins on time to progression for patients with high-risk PCa.
Patients with high- and very high risk PCa (NCCN definition of Gleason score ≥ 8, prostate-specific antigen (PSA) ≥ 20, or ≥cT3a) who received definitive RT at two institutions were included in this analysis. Progression was defined as either biochemical (PSA > nadir + 2 ng/mL), locoregional (prostate or lymph nodes, biopsy-proven), or development of distant metastases. Progression-free survival (PFS) was defined as the time elapsed from the start of RT to progression or last follow-up. Cox proportional hazards models evaluated the associations between non-oncologic medications and PFS.
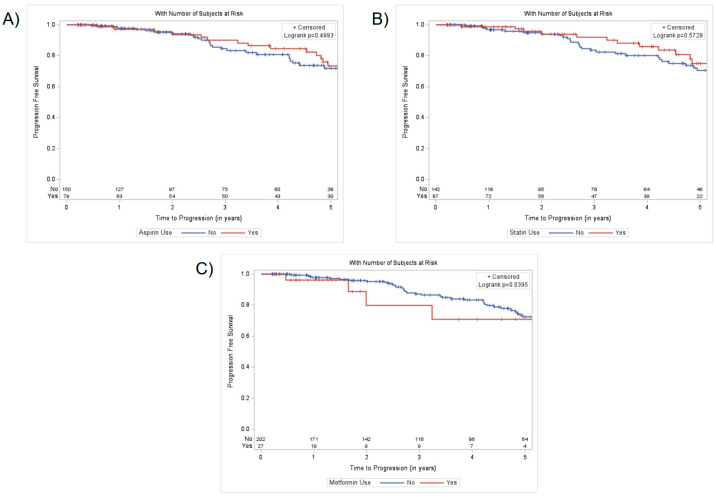
There were 237 patients eligible for this analysis, of which 47 (19.8%) and 178 (75.1%) had at least clinical T3 disease or at least Gleason 8 disease, respectively. During RT, 82 (34.6%), 88 (37.1%), and 29 (12.2%) patients were taking aspirin, statin, or metformin, respectively. Overall, 54 patients (22.8%) experienced disease progression. Neither aspirin nor statin usage had a significant association with PFS. Patients prescribed metformin displayed worse PFS compared to patients not taking metformin (aHR: 2.46, 95% CI: 1.06-5.72).
Aspirin and statin usage was not associated with likelihood of progression in this large cohort of patients with high-/very high risk PCa. Metformin use was associated with poorer PFS, albeit with a small event rate due to fewer patients taking metformin. Further studies are needed to clarify the impact of common non-oncologic medication use on outcomes for patients with high-risk PCa.
前列腺癌(PCa)放疗(RT)的治疗效果可能会受到非肿瘤药物同时使用的意外影响。许多研究已将几种非肿瘤药物的摄入与癌症特定结局联系起来。在本研究中,我们报告了包括阿司匹林、二甲双胍和他汀类药物在内的日常非肿瘤药物对高危PCa患者疾病进展时间的影响。
本分析纳入了在两个机构接受根治性放疗的高危和极高危PCa患者(根据美国国立综合癌症网络(NCCN)定义, Gleason评分≥8、前列腺特异性抗原(PSA)≥20或≥cT3a)。疾病进展定义为生化进展(PSA>最低点+2 ng/mL)、局部区域进展(前列腺或淋巴结,活检证实)或远处转移的发生。无进展生存期(PFS)定义为从放疗开始到疾病进展或最后一次随访的时间。Cox比例风险模型评估了非肿瘤药物与PFS之间的关联。
有237例患者符合本分析条件,其中分别有47例(19.8%)和178例(75.1%)至少患有临床T3期疾病或至少患有Gleason 8期疾病。在放疗期间,分别有82例(34.6%)、88例(37.1%)和29例(12.2%)患者服用阿司匹林、他汀类药物或二甲双胍。总体而言,54例患者(22.8%)出现疾病进展。服用阿司匹林和他汀类药物均与PFS无显著关联。与未服用二甲双胍的患者相比,服用二甲双胍的患者PFS更差(调整后风险比:2.46,95%置信区间:1.06 - 5.72)。
在这一大型高危/极高危PCa患者队列中,服用阿司匹林和他汀类药物与疾病进展的可能性无关。使用二甲双胍与较差的PFS相关,尽管由于服用二甲双胍的患者较少,事件发生率较低。需要进一步研究以阐明常用非肿瘤药物的使用对高危PCa患者结局的影响。