Kalas Noémi, Szabó Verita, Vida Balázs, Tóth Zsófia, Lőczi Lotti, Sebők Barbara, Merkely Petra, Lintner Balázs, Ács Nándor, Keszthelyi Attila, Várbíró Szabolcs, Tóth Richárd, Keszthelyi Márton
Department of Obstetrics and Gynecology, Semmelweis University, 1082 Budapest, Hungary.
Workgroup of Research Management, Doctoral School, Semmelweis University, 1085 Budapest, Hungary.
Life (Basel). 2025 Jun 18;15(6):971. doi: 10.3390/life15060971.
Cervical cancer continues to pose a significant global health challenge, particularly in low-resource regions with limited access to advanced diagnostics. Cervical conization can occasionally uncover invasive carcinoma in patients initially suspected of having only pre-invasive lesions. This study assessed the platelet-to-lymphocyte ratio (PLR) as a potential predictive biomarker for identifying invasive disease in patients undergoing a loop electrosurgical excision procedure (LEEP).
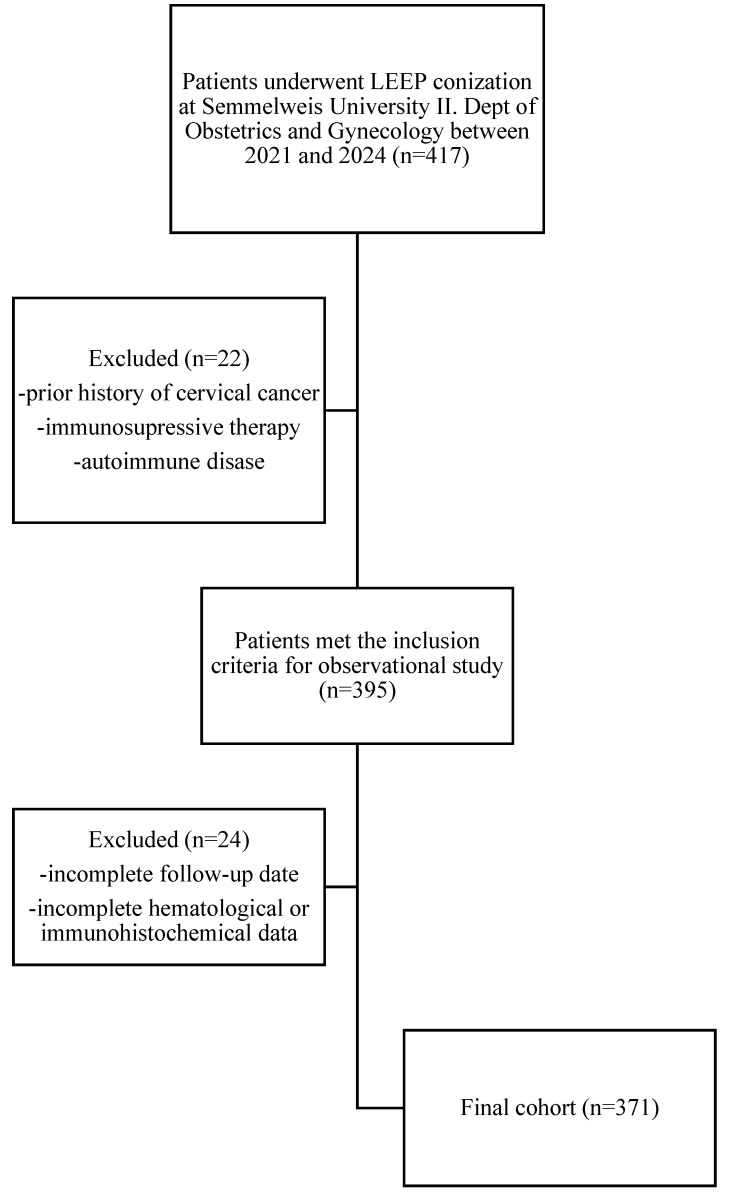
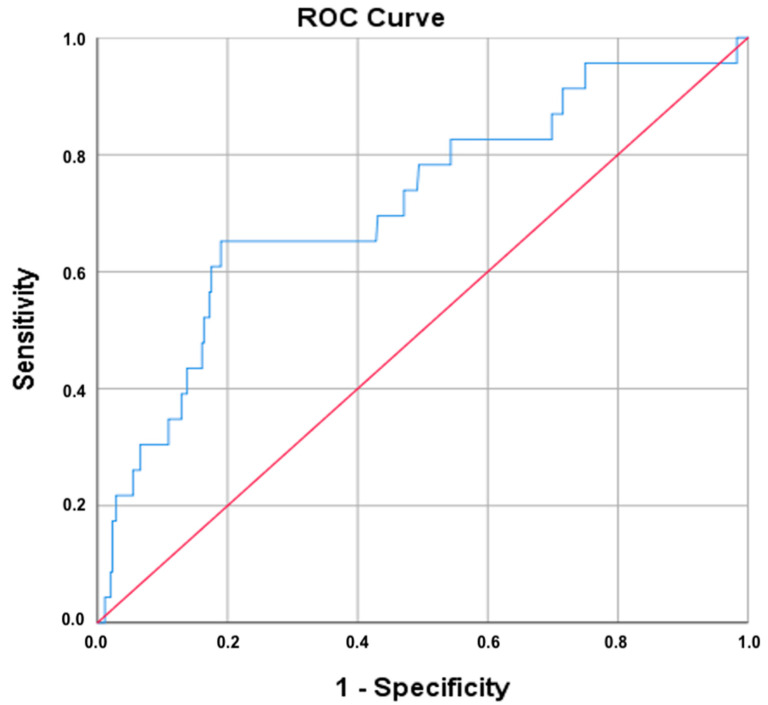
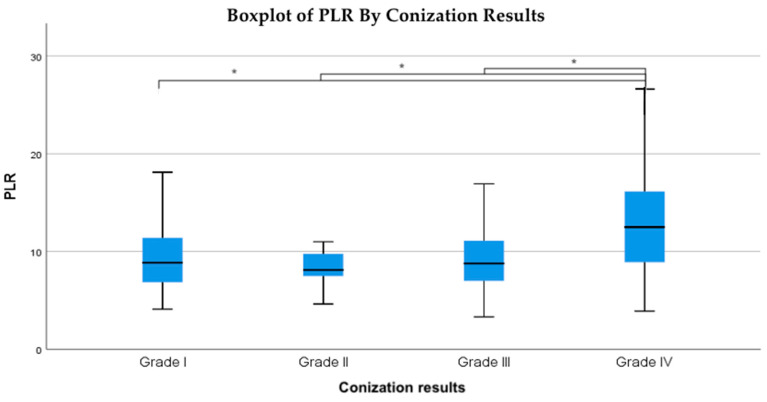
A retrospective study was conducted on 371 patients who underwent LEEP conization for cervical dysplasia. Preoperative PLR values were collected and compared across final histopathological categories (negative, low-grade, high-grade, invasive carcinoma) using the Kruskal-Wallis test, followed by Mann-Whitney U tests for pairwise comparisons. Receiver operating characteristic (ROC) analysis was used to evaluate diagnostic accuracy.
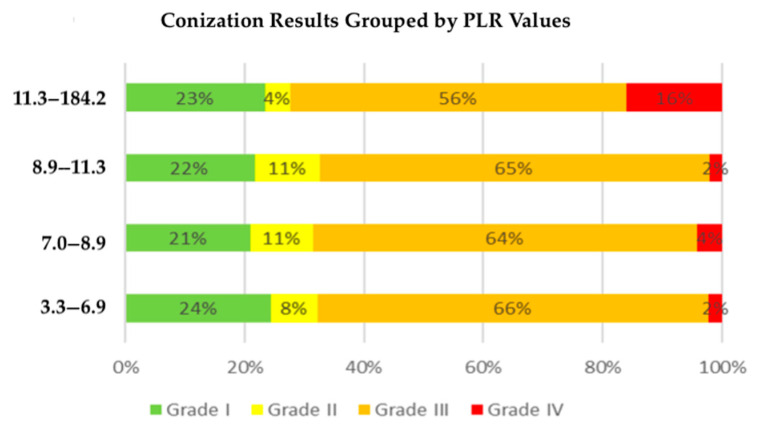
PLR values above 7.7 were significantly associated with HPV positivity, increasing with histopathological severity. There were significant PLR differences across the outcome groups ( = 0.005), with notably higher values in cases of invasive carcinoma ( < 0.01). ROC analysis showed moderate diagnostic utility (AUC ≈ 0.72); at a PLR cutoff of ~11.9, sensitivity was 65% and specificity 81%.
The PLR cutoff of 7.7 was associated with HPV positivity, while a higher cutoff of 11.93 was identified for predicting invasive cervical cancer. These findings support that preoperative PLR is a non-invasive, clinically relevant marker correlated with lesion severity, offering potential for preoperative risk stratification, particularly where advanced diagnostics are limited.
宫颈癌仍然是一项重大的全球健康挑战,尤其是在难以获得先进诊断技术的资源匮乏地区。宫颈锥切术偶尔会在最初仅怀疑有癌前病变的患者中发现浸润性癌。本研究评估了血小板与淋巴细胞比值(PLR)作为一种潜在的预测生物标志物,用于识别接受环形电切术(LEEP)的患者中的浸润性疾病。
对371例因宫颈发育异常接受LEEP锥切术的患者进行了一项回顾性研究。收集术前PLR值,并使用Kruskal-Wallis检验对最终组织病理学类别(阴性、低级别、高级别、浸润性癌)进行比较,随后使用Mann-Whitney U检验进行两两比较。采用受试者工作特征(ROC)分析来评估诊断准确性。
PLR值高于7.7与HPV阳性显著相关,并随组织病理学严重程度增加。各结局组之间的PLR存在显著差异(P = 0.005),浸润性癌病例中的PLR值明显更高(P < 0.01)。ROC分析显示具有中等诊断效用(AUC≈0.72);在PLR临界值约为11.9时,敏感性为65%,特异性为81%。
PLR临界值7.7与HPV阳性相关,而预测浸润性宫颈癌的较高临界值为11.93。这些发现支持术前PLR是一种与病变严重程度相关的非侵入性、临床相关标志物,为术前风险分层提供了可能性,特别是在先进诊断技术有限的情况下。