Svendsen Ann-Kristine Mandøe, Hagstrøm Søren, Thorsteinsson Kristina, Van Batavia Jason, Kamperis Konstantinos, Olesen Anne Estrup, Borch Luise
Department of Pediatrics and Adolescent Medicine, Gødstrup Hospital, Herning, Denmark.
NIDO, Centre for Research and Education, Gødstrup Hospital, Herning, Denmark.
JMIR Res Protoc. 2025 Jun 26;14:e63588. doi: 10.2196/63588.
According to International Children's Continence Society, the first-line treatment of children with daytime urinary incontinence is standard urotherapy, eventually followed by pharmacotherapy of anticholinergics. The effect of medical treatment is sparsely investigated and has been investigated primarily in nonrandomized trials.
The primary objective of this trial is to evaluate if (1) combination therapy of solifenacin and mirabegron in low doses is superior to monotherapy of solifenacin in high dose and if (2) combination therapy of mirabegron and solifenacin in low doses is superior to monotherapy of mirabegron in high dose in the treatment of daytime urinary incontinence among children aged 5-14 years who are noncomplete responders to monotherapy of solifenacin in low dose or monotherapy of mirabegron in low dose. The secondary objective is to evaluate the treatment response of combination therapy of solifenacin and mirabegron in low doses, monotherapy in high doses, and monotherapy in low doses as supplementary comparisons. Additionally, the secondary objective is to evaluate the side effects, safety, and tolerability of the medical treatment as well as the effect of the treatment on the well-being and quality of life.
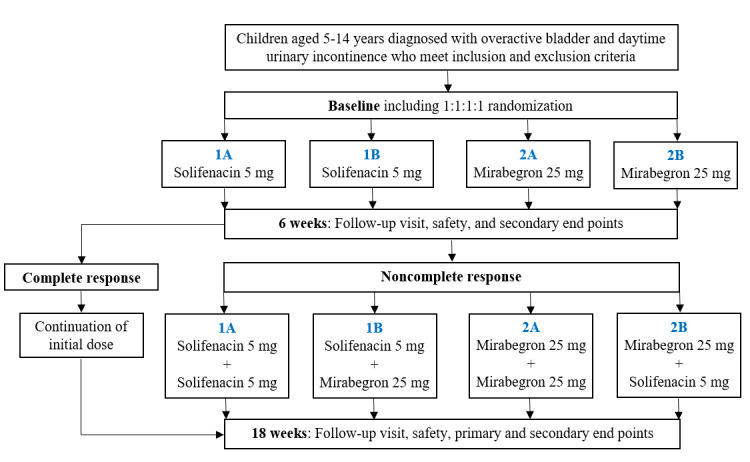
Children aged 5-14 years diagnosed with daytime urinary incontinence refractory to standard urotherapy will be randomized 1:1:1:1 to 4 treatment groups. Initially, 2 groups will receive solifenacin 5 mg and 2 groups will receive mirabegron 25 mg. After 6 weeks, noncomplete responders will receive add-on treatments according to their primary randomization group. Group 1A will receive solifenacin 5 mg and add-on solifenacin 5 mg, group 1B will receive solifenacin 5 mg and add-on mirabegron 25 mg, group 2A will receive mirabegron 25 mg and add-on mirabegron 25 mg, and group 2B will receive mirabegron 25 mg and add-on solifenacin 5 mg. The total treatment period will be 18 weeks. The primary end point measure is treatment response assessed by change from visit 2 to the end of the study, according to the number of wet days per 7 days by DryPie.
The BeDry study was approved by Clinical Trials in the European Union on June 12, 2024. Recruitment began on June 27, 2024, and will continue until 236 patients are included, which is expected to occur by September 2026. As of April 2025, 75 participants are included.
This trial has the potential to optimize the medical treatment of children with daytime urinary incontinence, shorten the treatment period, diminish the side effects, and minimize unnecessary medical expenses.
Clinical Trials in the European Union EUCT 2023-510187-13-00; https://tinyurl.com/2hva7ph8; ClinicalTrials.gov NCT06551246; https://clinicaltrials.gov/study/NCT06551246.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): PRR1-10.2196/63588.
根据国际儿童尿控协会的说法,儿童日间尿失禁的一线治疗是标准的尿疗法,最终可采用抗胆碱能药物进行药物治疗。药物治疗的效果研究较少,主要在非随机试验中进行了研究。
本试验的主要目的是评估:(1)低剂量索利那新和米拉贝隆联合治疗是否优于高剂量索利那新单药治疗;(2)低剂量米拉贝隆和索利那新联合治疗是否优于高剂量米拉贝隆单药治疗,用于治疗5至14岁对低剂量索利那新单药治疗或低剂量米拉贝隆单药治疗反应不完全的儿童日间尿失禁。次要目的是评估低剂量索利那新和米拉贝隆联合治疗、高剂量单药治疗和低剂量单药治疗作为补充比较的治疗反应。此外,次要目的是评估药物治疗的副作用、安全性和耐受性,以及治疗对幸福感和生活质量的影响。
诊断为对标准尿疗法难治的5至14岁儿童日间尿失禁患者将按1:1:1:1随机分为4个治疗组。最初,2组接受5毫克索利那新,2组接受25毫克米拉贝隆。6周后,反应不完全的患者将根据其初始随机分组接受追加治疗。1A组将接受5毫克索利那新并追加5毫克索利那新,1B组将接受5毫克索利那新并追加25毫克米拉贝隆,2A组将接受25毫克米拉贝隆并追加25毫克米拉贝隆,2B组将接受25毫克米拉贝隆并追加5毫克索利那新。总治疗期为18周。主要终点指标是根据DryPie每7天记录的尿床天数,通过从第2次就诊到研究结束时的变化来评估治疗反应。
BeDry研究于2024年6月12日获得欧盟临床试验批准。招募工作于2024年6月27日开始,将持续到纳入236名患者,预计将于2026年9月完成。截至2025年4月,已纳入75名参与者。
本试验有可能优化儿童日间尿失禁的药物治疗,缩短治疗周期,减少副作用,并将不必要的医疗费用降至最低。
欧盟临床试验EUCT 2023 - 510187 - 13 - 00;https://tinyurl.com/2hva7ph8;美国国立医学图书馆临床试验注册中心NCT06551246;https://clinicaltrials.gov/study/NCT06551246。
国际注册报告识别码(IRRID):PRR1 - 10.2196 / 63588。