Manikpurage Hasanga D, Bourgault Jérôme, Houessou Ursula, Paulin Audrey, Zamani Pardis, Gagnon Eloi, Li Zhonglin, Boudreau Dominique K, Eslami Aida, Voisine Pierre, Mathieu Patrick, Bossé Yohan, Arsenault Benoit J, Thériault Sébastien
Centre de Recherche de l'Institut Universitaire de Cardiologie et de Pneumologie de Québec - Université Laval, Québec, QC, Canada.
Department of Social and Preventive Medicine, Faculty of Medicine, Université Laval, Québec, QC, Canada.
Commun Med (Lond). 2025 Jul 1;5(1):264. doi: 10.1038/s43856-025-00981-w.
Polygenic risk scores (PRS) could help to identify individuals with a high genetic risk profile for coronary artery disease (CAD). We aimed to evaluate the association between previously reported PRS and myocardial infarction (MI) as well as the extent and recurrence of coronary artery lesions.
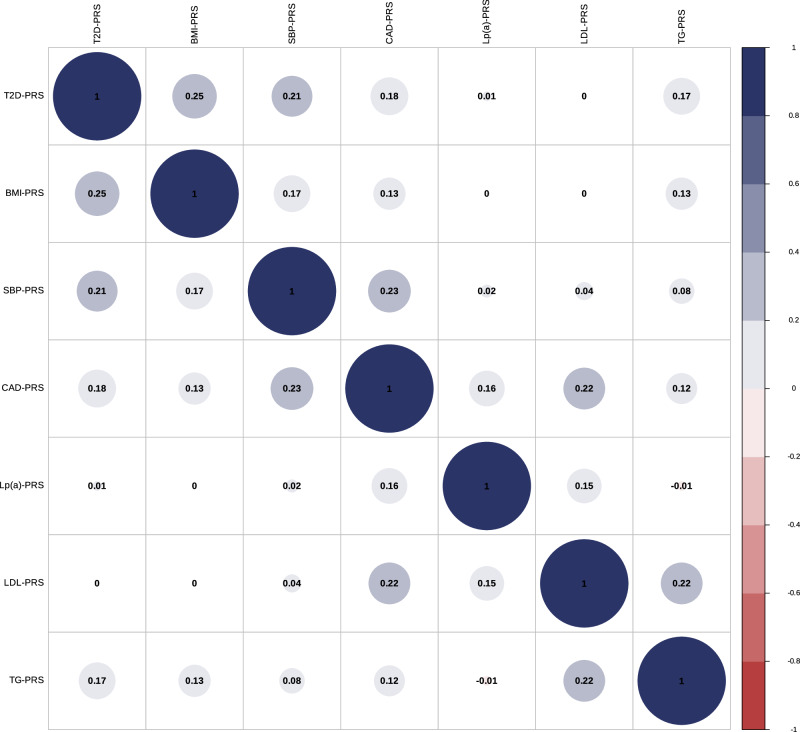
We validated previously reported CAD-PRS and 6 cardiovascular (CV) risk factors PRS (systolic blood pressure [SBP], type 2 diabetes [T2D], body-mass index [BMI], low-density lipoprotein cholesterol [LDL], triglycerides [TG], and lipoprotein-[a][Lp(a)]) in individuals of European ancestry from two Canadian population-based cohorts, the Canadian Longitudinal Study on Aging (CLSA, N = 24,599) and CARTaGENE (N = 26,806). Using a stepwise model, we determined an optimal combination of PRS to identify MI. We tested the selected PRS for association with the severity and recurrence of atherosclerotic CAD evaluated by coronary angiography in patients undergoing cardiac surgery (QUEBEC-ANGIO, N = 4108).
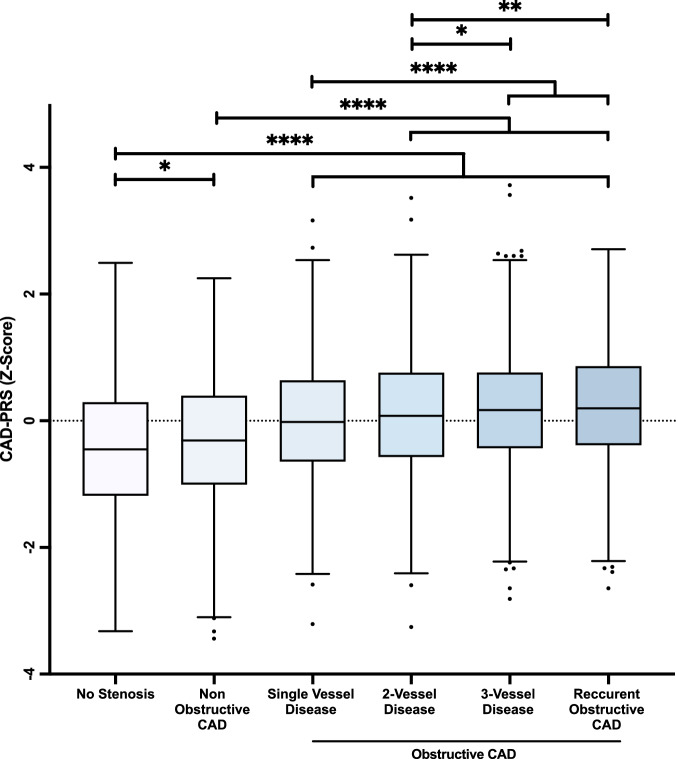
We show that the CAD-PRS most strongly associated with MI has odds ratios per standard deviation increment of 1.75 [1.64-1.86] (P = 1.57E-70) in CLSA and 1.87 [1.73-2.03] (P = 3.06E-53) in CARTaGENE. In CLSA, the optimal model includes CAD-PRS, SBP-PRS, BMI-PRS, LDL-PRS, TG-PRS and Lp(a)-PRS. Adding these PRS increases modestly yet significantly the discriminative capacity when compared to traditional risk factors (difference of AUC = 0.025 [0.019-0.031] in CLSA, 0.018 [0.012-0.024] in CARTaGENE). In QUEBEC-ANGIO, the CAD-PRS is gradually and significantly associated with the extent and recurrence of CAD.
Screening multiple validated PRS may significantly improve genetic risk estimation of MI as well as the extent and recurrence of coronary artery lesions.
多基因风险评分(PRS)有助于识别冠状动脉疾病(CAD)遗传风险较高的个体。我们旨在评估先前报道的PRS与心肌梗死(MI)之间的关联,以及冠状动脉病变的程度和复发情况。
我们在来自加拿大两个基于人群队列的欧洲血统个体中验证了先前报道的CAD-PRS和6种心血管(CV)危险因素PRS(收缩压[SBP]、2型糖尿病[T2D]、体重指数[BMI]、低密度脂蛋白胆固醇[LDL]、甘油三酯[TG]和脂蛋白[a][Lp(a)]),即加拿大老龄化纵向研究(CLSA,N = 24,599)和CARTaGENE(N = 26,806)。使用逐步模型,我们确定了用于识别MI的PRS的最佳组合。我们在接受心脏手术的患者(魁北克血管造影研究,N = 4108)中测试了所选PRS与通过冠状动脉造影评估的动脉粥样硬化性CAD的严重程度和复发之间的关联。
我们发现,与MI最密切相关的CAD-PRS在CLSA中每标准差增加的比值比为1.75[1.64 - 1.86](P = 1.57E-70),在CARTaGENE中为1.87[1.73 - 2.03](P = 3.06E-53)。在CLSA中,最佳模型包括CAD-PRS、SBP-PRS、BMI-PRS、LDL-PRS、TG-PRS和Lp(a)-PRS。与传统危险因素相比,添加这些PRS可适度但显著提高判别能力(CLSA中AUC差异为0.025[0.019 - 0.031],CARTaGENE中为0.018[0.012 - 0.024])。在魁北克血管造影研究中,CAD-PRS与CAD的程度和复发逐渐且显著相关。
筛查多个经过验证的PRS可能会显著改善MI的遗传风险估计以及冠状动脉病变的程度和复发情况。