Panda Sushree Nibedita, Barik Manish, Ratna P, Das Prabhu Kalyan
The George Institute for Global Health, Hyderabad, India.
Independent researcher, Delhi, India.
Trop Med Health. 2025 Jul 11;53(1):92. doi: 10.1186/s41182-025-00752-2.
Shaped by its colonial origins, tropical medicine sustains inequitable power dynamics in global health, sidelining low-middle-income countries (LMICs) in critical decision-making processes over research agendas and priorities. Editorial boards of tropical medicine journals, dominated by scholars from high-income countries (HICs), risk reinforcing power imbalances and excluding context-driven expertise from endemic regions. This study examines the diversity of editorial boards across gender, geographic, socioeconomic, and geopolitical dimensions to assess systemic inequities.
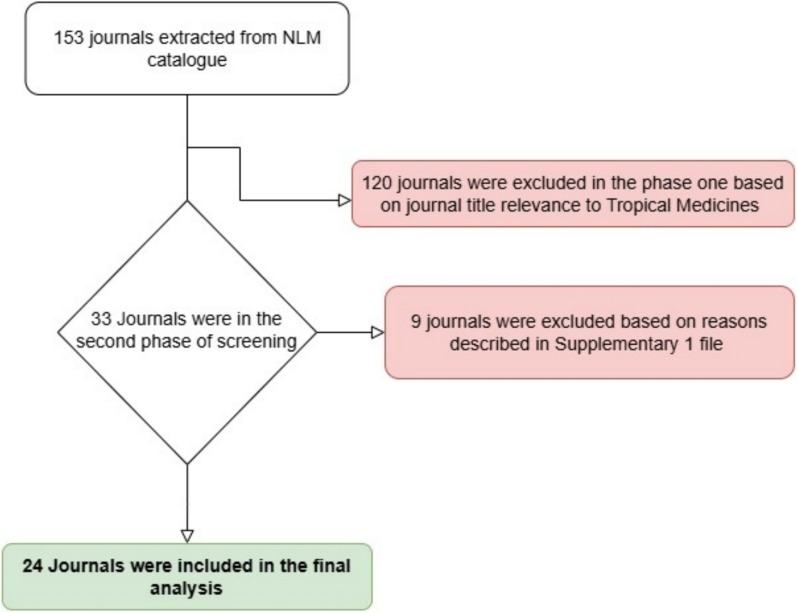
A systematic search of the National Library of Medicine (NLM) catalog was conducted via a targeted strategy between October and December 2024. After screening 153 journals for title relevance and applying exclusion criteria based on publication status, availability of editorial information, and global scope, 24 journals were selected. Data on 2,226 editorial board members were extracted from journal and institutional websites. Data on gender, country of affiliation (classified by World Bank income/regions), and geopolitical groups (G7, G20, BRICS) were extracted from public sources. Gender determination used a sequential approach (journal descriptions, Genderize.io, and consensus). Descriptive statistics were used to perform the analysis.
The editorial board comprised 2,226 members, 66% male, 31.2% female, and 2.8% undetermined, from 120 nations. The regional contributions included Europe and Central Asia (21.9%), North America (20.9%), East Asia and the Pacific (16.6%), and Latin America and the Caribbean (16.2%), whereas Sub-Saharan Africa (11.2%), South Asia (9.7%), and the Middle East and North Africa (3.4%) were underrepresented. Over half (52.8%) were affiliated with high-income countries. Geopolitically, 40.3% were from the G7, 67.1% were from the G20, and 24.2% were from the BRICS. Some journals showed skewing, with 85.2% North American representation and 90.3% East Asia-Pacific dominance.
Tropical medicine editorial boards are steeped in systemic inequities that echo colonial legacies, with the overrepresentation of HICs and men limiting LMIC perspectives and local expertise. This imbalance undermines research relevance and ethical integrity by prioritizing Global North agendas over the needs of populations most affected by tropical diseases. To address these disparities, substantial reforms are essential. Strategies such as instituting DEI (Diversity, Equity and Inclusion), creating targeted mentorship programs for LMIC researchers, and enforcing transparent, bias-resistant recruitment practices are important. Such measures will create a more inclusive editorial landscape that aligns research priorities with global health needs, promoting equitable and contextually relevant solutions.
受其殖民起源的影响,热带医学在全球卫生领域维持着不公平的权力动态,在研究议程和优先事项的关键决策过程中,将中低收入国家(LMICs)边缘化。热带医学期刊的编辑委员会由高收入国家(HICs)的学者主导,有可能加剧权力失衡,并将来自流行地区的因地制宜的专业知识排除在外。本研究从性别、地理、社会经济和地缘政治维度审视编辑委员会的多样性,以评估系统性不平等。
2024年10月至12月期间,通过有针对性的策略对美国国立医学图书馆(NLM)目录进行了系统检索。在筛选了153种期刊的标题相关性,并根据出版状态、编辑信息的可用性和全球范围应用排除标准后,选择了24种期刊。从期刊和机构网站提取了2226名编辑委员会成员的数据。从公共来源提取了性别、所属国家(按世界银行收入/地区分类)和地缘政治集团(G7、G20、金砖国家)的数据。性别确定采用了循序渐进的方法(期刊描述、Genderize.io和达成共识)。使用描述性统计进行分析。
编辑委员会由来自120个国家的2226名成员组成,其中男性占66%,女性占31.2%,未确定性别者占2.8%。区域贡献包括欧洲和中亚(21.9%)、北美(20.9%)、东亚和太平洋(16.6%)以及拉丁美洲和加勒比(16.2%),而撒哈拉以南非洲(11.2%)、南亚(9.7%)和中东及北非(3.4%)的代表性不足。超过一半(52.8%)的成员隶属于高收入国家。在地缘政治方面,40.3%来自G7,67.1%来自G20,24.2%来自金砖国家。一些期刊存在偏差,北美代表占85.2%,东亚-太平洋占主导地位达90.3%。
热带医学编辑委员会深陷系统性不平等之中,这反映了殖民遗产,高收入国家和男性的代表性过高,限制了中低收入国家的观点和当地专业知识。这种不平衡通过将全球北方的议程置于受热带疾病影响最严重人群的需求之上,损害了研究的相关性和道德完整性。为解决这些差距,进行实质性改革至关重要。诸如实施多元化、公平和包容(DEI)、为中低收入国家的研究人员创建有针对性的指导计划以及实施透明、抗偏见的招聘做法等策略很重要。这些措施将创造一个更具包容性的编辑格局,使研究重点与全球卫生需求相一致,并促进公平且因地制宜的解决方案。