Faucher Marion, Ravot Stanislas, Barthes Loïc, de Guibert Jean Manuel, Chow-Chine Laurent, Gonzalez Frédéric, Bisbal Magali, Servan Luca, Tezier Marie, Tourret Maxime, Cambon Sylvie, Pouliquen Camille, Mallet Damien, Nguyen Duong Lam, Ettori Florence, Ewald Jacques, Léone Marc, Sannini Antoine, Garnier Jonathan, Mokart Djamel
Department of Anesthesiology and Critical Care, Paoli-Calmettes Institute, 13009 Marseille, France.
Department of Surgery, Paoli-Calmettes Institute, 13009 Marseille, France.
Cancers (Basel). 2025 Jul 4;17(13):2241. doi: 10.3390/cancers17132241.
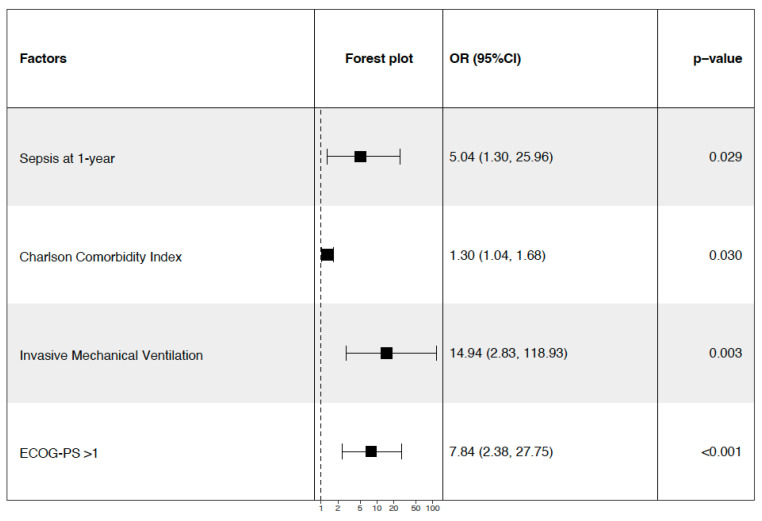
Splenectomy remains necessary in selected oncologic and hematologic indications but is associated with significant postoperative morbidity and mortality. The data on outcomes in this high-risk population remain limited, particularly in mixed cohorts. : We conducted a retrospective cohort study including all patients undergoing splenectomy for oncologic or hematologic causes between 2009 and 2022 at a cancer referral center. The primary outcomes were the occurrence of major complications at day 90 and the 1-year all-cause mortality. Multivariate logistic regression was used to identify independent predictors. Among the 8503 ICU admissions from surgical wards, 204 splenectomies were performed; 179 patients were analyzed. The median age was 64 years, and 100 patients (55.9%) were female. Splenectomy was performed for hematologic malignancies in 76 cases (42.5%) and for oncologic causes in 103 cases (57.5%). Laparotomy was used in 154 cases (86.0%), and metastasectomy was performed in 54 patients (30.2%). At day 90, 86 patients (48.0%) developed a major complication: 12 deaths (6.7%), 44 surgical complications (24.6%), and 71 episodes of sepsis (39.7%). In a multivariate analysis, weight loss (OR 3.39, 95% CI [1.32-8.70], = 0.011), laparotomy (OR 4.38 [1.09-17.60], = 0.038), and a higher SAPS II score (OR 1.08 per point [1.03-1.13], = 0.003) were associated with complications, while metastasectomy was protective (OR 0.23 [0.08-0.67], = 0.007). At one year, the mortality reached 22.4%. Independent predictors of death were sepsis at one year (OR 5.04, 95% CI [1.30-25.96], = 0.029), the Charlson Comorbidity Index (OR 1.30 per point, 95% CI [1.04-1.68], = 0.030), invasive mechanical ventilation (OR 14.94, 95% CI [2.83-118.93], = 0.003), and a performance status >1 (OR 7.84, 95% CI [2.38-27.75], < 0.001). Encapsulated bacteria were not isolated; sepsis was mainly due to Gram-negative and enterococcal organisms. : Splenectomy in onco-hematologic patients is associated with high rates of sepsis and mortality. In addition to surgical factors, frailty, immune status, and infection independently contribute to the patients' outcomes. These results support risk-adapted perioperative strategies and long-term infectious surveillance in immunocompromised patients.
在特定的肿瘤学和血液学适应症中,脾切除术仍然是必要的,但它与显著的术后发病率和死亡率相关。关于这个高风险人群的预后数据仍然有限,尤其是在混合队列中。我们进行了一项回顾性队列研究,纳入了2009年至2022年期间在一家癌症转诊中心因肿瘤学或血液学原因接受脾切除术的所有患者。主要结局是90天时主要并发症的发生情况和1年全因死亡率。采用多因素逻辑回归来确定独立预测因素。在来自外科病房的8503例重症监护病房入院患者中,进行了204例脾切除术;对179例患者进行了分析。中位年龄为64岁,100例患者(55.9%)为女性。76例(42.5%)因血液系统恶性肿瘤进行脾切除术,103例(57.5%)因肿瘤学原因进行脾切除术。154例(86.0%)采用剖腹手术,54例患者(30.2%)进行了转移灶切除术。在90天时,86例患者(48.0%)发生了主要并发症:12例死亡(6.7%),44例手术并发症(24.6%),71例脓毒症发作(39.7%)。在多因素分析中,体重减轻(比值比3.39,95%置信区间[1.32 - 8.70],P = 0.011)、剖腹手术(比值比4.38[1.09 - 17.60],P = 0.038)和较高的简化急性生理学评分II(SAPS II)(每增加1分比值比1.08[1.03 - 1.13],P = 0.003)与并发症相关,而转移灶切除术具有保护作用(比值比0.23[0.08 - 0.67],P = 0.007)。在1年时,死亡率达到22.4%。死亡的独立预测因素是1年时的脓毒症(比值比5.04,95%置信区间[1.30 - 25.96],P = 0.029)、查尔森合并症指数(每增加1分比值比1.30,95%置信区间[1.04 - 1.68],P = 0.030)、有创机械通气(比值比14.94,95%置信区间[2.83 - 118.93],P = 0.003)和体能状态>1(比值比7.84,95%置信区间[2.38 - 27.75],P < 0.001)。未分离出包膜细菌;脓毒症主要由革兰氏阴性菌和肠球菌引起。肿瘤血液学患者的脾切除术与高脓毒症发生率和死亡率相关。除手术因素外,虚弱、免疫状态和感染独立影响患者的预后。这些结果支持在免疫功能低下患者中采用风险适应性围手术期策略和长期感染监测。