Ilfeld Brian M, Abramson Wendy B, Said Engy T, Sztain Jacklynn F, Finneran John J, Griggs Jonna L, Abdullah Baharin, Jensen Evan J, Schaar Adam, Wallace Anne M
Department of Anesthesiology, University California San Diego, San Diego, California, USA.
Department of Surgery, University California San Diego, San Diego, California, USA.
Can J Pain. 2025 Jul 10;9(1):2521117. doi: 10.1080/24740527.2025.2521117. eCollection 2025.
Percutaneous auricular neuromodulation involves implanting electrodes around the ear and administering an electric current. A device is currently available that is cleared to treat symptoms from opioid withdrawal, and multiple reports suggest a possible postoperative analgesic effect. This randomized, controlled pilot study aimed to (1) assess the feasibility of a postoperative auricular neuromodulation protocol and (2) provide an estimate of its treatment effects on postoperative pain and opioid consumption.
Adults undergoing unilateral or bilateral ambulatory breast surgery with anticipated moderate-severe pain and a single-injection paravertebral nerve block(s) received an auricular neuromodulation device (NSS-2 Bridge, Masimo) following surgery. Participants were randomized to 5 days of electrical stimulation or sham in a double-masked fashion.
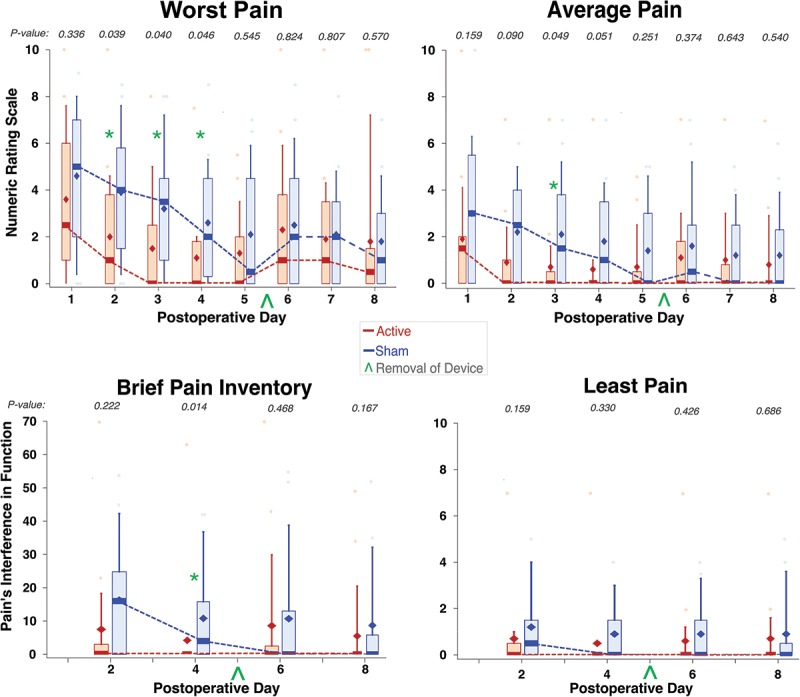
In the first 5 days, the median pain for those receiving active stimulation ( = 15) was 0 (interquartile range [IQR] = 0, 0.5] versus 1.5 (IQR = 0, 3.8) for the sham group ( = 15, = 0.084). Concurrently, the median oxycodone use for active stimulation was 0 mg (IQR = 0, 2.5) compared to 0 mg (IQR = 0, 3) for the sham group ( = 0.905). Various secondary outcomes reached statistical significance, including maximum and average daily pain scores.
This pilot study demonstrates that percutaneous auricular neuromodulation is a feasible approach for managing pain in ambulatory surgical procedures and shows potential as an effective analgesic following discharge. Considering its ease of application, absence of systemic side effects, and lack of significant complications, conducting a definitive clinical trial seems justified because the current study was underpowered, which possibly resulted in the lack of statistical significance for the primary outcome.: Clinicaltrials.gov NCT05521516.
经皮耳神经调节术包括在耳朵周围植入电极并施加电流。目前有一种已获批用于治疗阿片类药物戒断症状的设备,多项报告表明其可能具有术后镇痛效果。这项随机对照试验性研究旨在:(1)评估术后耳神经调节方案的可行性;(2)估计其对术后疼痛和阿片类药物消耗量的治疗效果。
预计术后会出现中度至重度疼痛且接受单次注射椎旁神经阻滞的单侧或双侧门诊乳房手术成年患者,术后接受耳神经调节设备(NSS - 2 Bridge,Masimo)治疗。参与者以双盲方式随机分为接受5天电刺激组或假刺激组。
在最初5天,接受主动刺激的患者(n = 15)的疼痛中位数为0(四分位间距[IQR] = 0,0.5]),而假刺激组(n = 15)为1.5(IQR = 0,3.8)(P = 0.084)。同时,主动刺激组的羟考酮使用中位数为0 mg(IQR = 0,2.5),假刺激组为0 mg(IQR = 0,3)(P = 0.905)。包括最大和平均每日疼痛评分在内的各种次要结局达到统计学显著性。
这项试验性研究表明,经皮耳神经调节术是门诊手术疼痛管理的一种可行方法,并且显示出出院后作为有效镇痛方法的潜力。鉴于其应用简便、无全身副作用且无重大并发症,进行一项确定性临床试验似乎是合理的,因为当前研究的效能不足,这可能导致主要结局缺乏统计学显著性。:Clinicaltrials.gov NCT05521516