Song Bolun, Wang Liming, Chen Yinggang, Hirano Yasumitsu
Department of Gastrointestinal Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, China.
Division of Gastroenterological Surgery, Saitama Medical University International Medical Center, Saitama, Japan.
J Gastrointest Oncol. 2025 Jun 30;16(3):1001-1012. doi: 10.21037/jgo-2024-982. Epub 2025 Jun 23.
The prognosis of stage IIIA colorectal cancer (CRC) is much better than that of stage II CRC in Japan. This study aimed to investigate the clinical implications of lymph node metastasis (LNM) in patients with pT1-2 CRC and explore the potential for downstaging pT1-2N+ CRC.
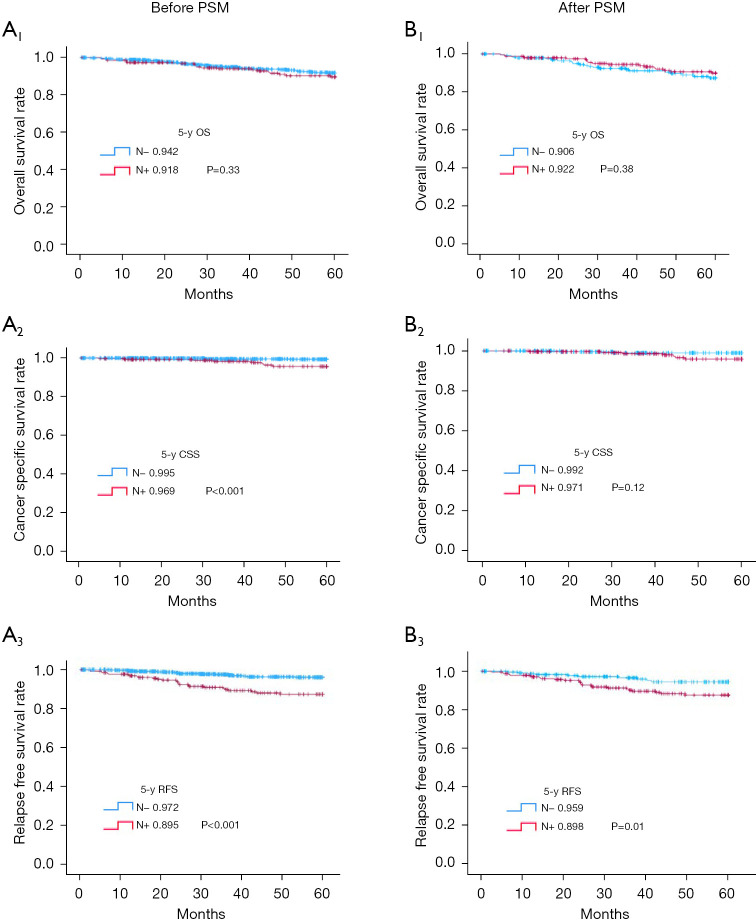
This retrospective cohort study took place at Saitama Medical University International Medical Center in Japan. We stratified patients with pT1-2 CRC (n=1,288) by presence (LNM+) or absence (LNM-) of LNM, assessing overall survival (OS), cancer-specific survival (CSS), and relapse-free survival (RFS) in both groups before and after propensity score matching (PSM). Cox multivariate analysis served for screening of prognostic risk factors.
LNM+ was ultimately confirmed in 256 study subjects (19.9%). Before matching, tumors of the LNM+ (. LNM-) group were more inclined to be large (≥2 cm: 76.6% . 61.2%; P<0.001), with greater propensity for infiltrating or ulcerative features (55.1% . 36.2%; P<0.001) and histotypes of lesser differentiation (moderately differentiated adenocarcinoma/poorly differentiated adenocarcinoma/signet-ring carcinoma/mucinous carcinoma: 65.6% . 45.8%; P<0.001). Likewise, they showed greater tendency for aggressive growth (91.0% . 81.1%; P<001), lymphatic (44.5% . 19.4%; P<0.001) or vascular (59.0% . 35.1%; P<0.001) invasion, and prolific lymph node harvesting (23.6±12.2 . 21.7±12.3; P=0.02). Although similar in terms of OS (LNM-, 94.2%; LNM+, 91.8%; P=0.33), the LNM- (. LNM+) group displayed significantly better CSS (99.5% . 96.9%; P<0.001) and RFS (97.2% . 89.5%; P<0.001). After matching, RFS still proved significantly better in the LNM- (. LNM+) group (95.9% . 89.8%; P=0.01), with multivariate analysis identifying LNM+ as an independent risk factor for RFS before and after PSM. A higher recurrence rate was also evident in the LNM+ (. LNM-) group [before matching: 10.5% . 2.8% (P<0.001); after matching: 10.2% . 4.1% (P=0.008)], involving liver and lymph nodes primarily. Neither OS nor CSS differed significantly by group.
LNM+ pT1-2 CRC patients had a higher risk of hepatic and nodal recurrence, but long-term OS and CSS were unaffected. Perhaps an appropriate downstaging of pT1-2N+ CRC from stage IIIA is a reasonable prospect.
在日本,ⅢA期结直肠癌(CRC)的预后比Ⅱ期CRC好得多。本研究旨在探讨pT1-2期CRC患者淋巴结转移(LNM)的临床意义,并探索降低pT1-2N+期CRC分期的可能性。
这项回顾性队列研究在日本埼玉医科大学国际医疗中心进行。我们根据有无LNM将pT1-2期CRC患者(n = 1288)分为两组,即LNM阳性(LNM+)组和LNM阴性(LNM-)组,在倾向评分匹配(PSM)前后评估两组的总生存期(OS)、癌症特异性生存期(CSS)和无复发生存期(RFS)。采用Cox多因素分析筛选预后危险因素。
最终在256例研究对象(19.9%)中确认存在LNM+。匹配前,LNM+(对LNM-)组的肿瘤更倾向于体积较大(≥2 cm:76.6%对61.2%;P<0.001),更倾向于具有浸润性或溃疡性特征(55.1%对36.2%;P<0.001)以及低分化组织学类型(中分化腺癌/低分化腺癌/印戒细胞癌/黏液癌:65.6%对45.8%;P<0.001)。同样,它们显示出更强的侵袭性生长倾向(91.0%对81.1%;P<0.01)、淋巴管(44.5%对19.4%;P<0.001)或血管(59.0%对35.1%;P<0.001)侵犯,以及更多的淋巴结清扫数量(23.6±12.2对21.7±12.3;P = 0.02)。尽管在OS方面相似(LNM-组为94.2%,LNM+组为91.8%;P = 0.33),但LNM-(对LNM+)组的CSS(99.5%对96.9%;P<0.001)和RFS(97.2%对89.5%;P<0.001)明显更好。匹配后,LNM-(对LNM+)组的RFS仍然明显更好(95.9%对89.8%;P = 0.01),多因素分析确定LNM+是PSM前后RFS的独立危险因素。LNM+(对LNM-)组的复发率也更高[匹配前:10.5%对2.8%(P<0.001);匹配后:10.2%对4.1%(P = 0.008)],主要累及肝脏和淋巴结。两组的OS和CSS均无显著差异。
LNM+的pT1-2期CRC患者肝转移和淋巴结复发风险较高,但长期OS和CSS不受影响。或许将pT1-2N+期CRC从ⅢA期进行适当降期是一个合理的前景。