Tengesdal Stig, Molberg Øyvind, Holme Øyvind, Gran Jan Tore, Myklebust Geirmund
Department of Research, Sorlandet Hospital, Egsveien 100, Kristiansand, 4615, Norway.
Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
Arthritis Res Ther. 2025 Jul 21;27(1):154. doi: 10.1186/s13075-025-03613-9.
Robust long-term mortality data on patients with polymyalgia rheumatica (PMR) are lacking. The aim of this study was to determine all-cause mortality in isolated PMR using a large, population-based, inception cohort followed prospectively over a 38-year period.
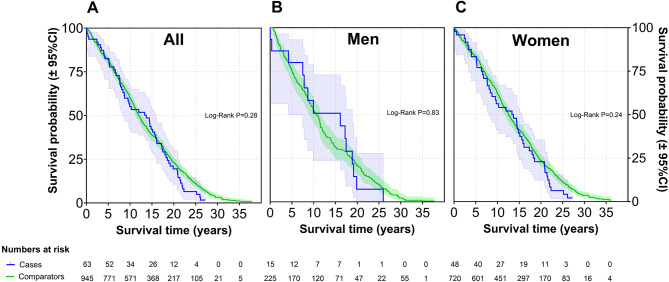
Between 1987 and 1997, 337 incident cases of PMR and biopsy-proven GCA were included in a prospective, population-based inception cohort in Aust-Agder County, Norway. Diagnosis was ascertained clinically by a rheumatologist, with PMR cases meeting Bird`s criteria. Patients were followed until death or end of study on December 31st, 2024. Each case was matched by gender, age at inclusion, and residency with 15 population comparators drawn from the population registry in Norway. We assessed mortality and survival by standard mortality ratios (SMR) and the Kaplan-Meier method.
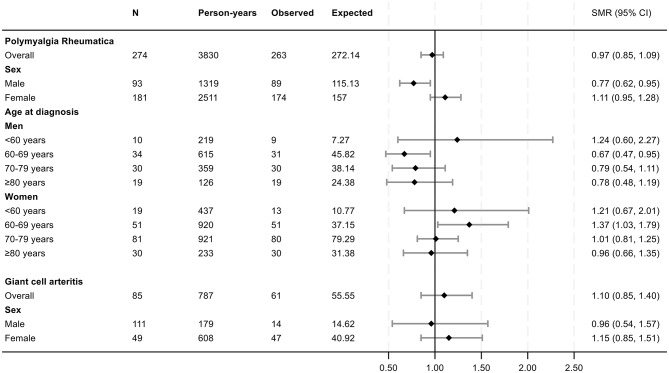
A total of 274 patients with isolated PMR (66.1% female, mean age at diagnosis 71.9 years) and 63 patients with GCA (76.2% female, mean age at diagnosis 71.6 years) were included. By the end of the study, 96.4% of all patients were deceased. Mean follow-up time for all patients was 13.7 years, with a maximum of 35.3 years. For cases with isolated PMR, the overall SMR was 0.97 (95% confidence interval [CI] 0.85, 1.09), for men 0.77 (95% CI 0.62, 0.95), and for women 1.11 (95% CI 0.95, 1.28). For GCA, the overall SMR was 1.10 (95% CI 0.85, 1.40), with no gender difference.
In this comprehensive long-term follow-up study with nearly complete data on mortality, isolated PMR was not associated with increased mortality, reinforcing the view that it does not confer a higher mortality risk.
目前缺乏关于风湿性多肌痛(PMR)患者的可靠长期死亡率数据。本研究的目的是利用一个基于人群的大型起始队列,前瞻性地随访38年,以确定孤立性PMR患者的全因死亡率。
1987年至1997年期间,挪威奥斯特-阿格德尔郡的一个基于人群的前瞻性起始队列纳入了337例PMR和经活检证实的巨细胞动脉炎(GCA)的新发病例。由风湿病学家进行临床诊断,PMR病例符合伯德标准。对患者进行随访直至死亡或2024年12月31日研究结束。每个病例按性别、纳入时年龄和居住地与从挪威人口登记处抽取的15名人群对照者进行匹配。我们通过标准化死亡率比(SMR)和Kaplan-Meier方法评估死亡率和生存率。
共纳入274例孤立性PMR患者(66.1%为女性,诊断时平均年龄71.9岁)和63例GCA患者(76.2%为女性,诊断时平均年龄71.6岁)。到研究结束时,所有患者中有96.4%死亡。所有患者的平均随访时间为13.7年,最长为35.3年。对于孤立性PMR病例,总体SMR为0.97(95%置信区间[CI]0.85,1.09),男性为0.77(95%CI0.62,0.95),女性为1.11(95%CI0.95,1.28)。对于GCA,总体SMR为1.10(95%CI0.85,1.40),无性别差异。
在这项关于死亡率数据几乎完整的全面长期随访研究中,孤立性PMR与死亡率增加无关,这进一步支持了它不会带来更高死亡风险的观点。