Yan Liyu, Wu Guishen
Department of Critical Care Medicine, Zhongshan People's Hospital, Zhongshan, China.
Front Med (Lausanne). 2025 Jul 8;12:1594128. doi: 10.3389/fmed.2025.1594128. eCollection 2025.
The purpose of this study is to compare different non-invasive respiratory support methods for the treatment of acute hypercapnic respiratory failure (AHRF).
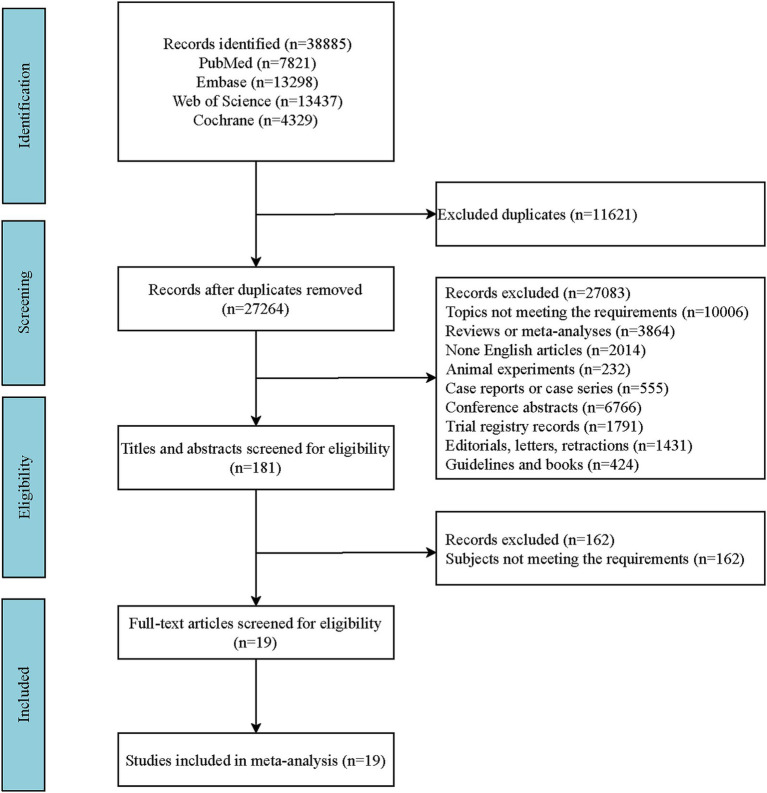
The network meta-analysis was conducted based on studies from PubMed, Embase, the Cochrane Library, and Web of Science, from their inception to September 10, 2024. The outcomes was treatment failure, all-cause mortality, intubation, dyspnea score, length of stay in hospital, respiratory rate, arterial carbon dioxide partial pressure (PaCO), and complications. The results of both direct and indirect comparisons were quantitatively assessed using weighted mean differences or relative risks with their respective 95% confidence intervals, and graphically depicted in forest plots. Additionally, the rank probabilities were presented, demonstrating the likelihood of each non-invasive respiratory support method being the most effective across various measured outcomes.
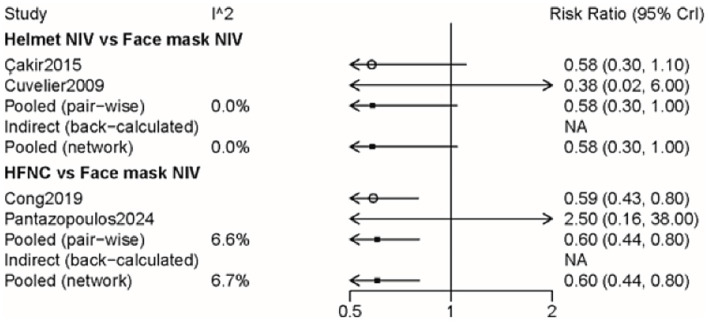
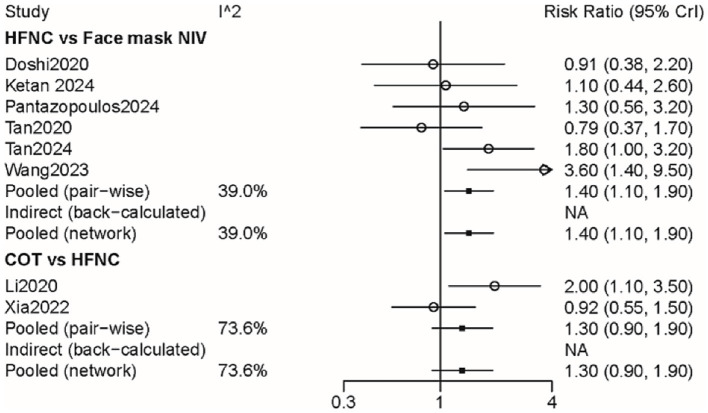
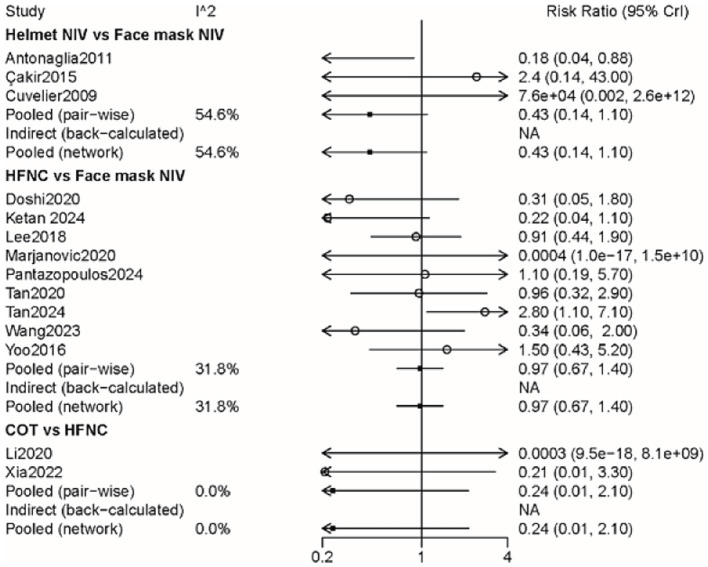
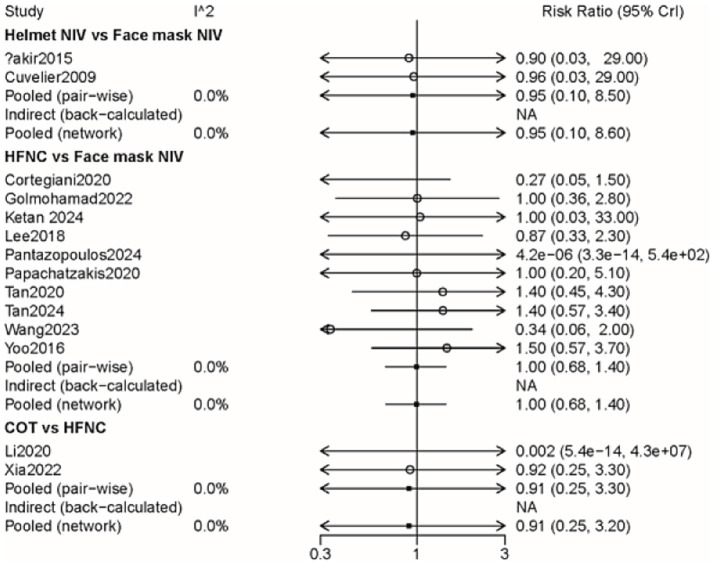
Nineteen studies (2,022 participants) were included. The results indicated that the probability of treatment failure with face mask non-invasive ventilation (NIV) was lower than that of high-flow nasal cannula (HFNC) (RR: 1.42, 95% CI: 1.06, 1.93) and conventional oxygen treatment (COT) (RR: 1.87, 95% CI: 1.16, 3.03). Face mask NIV demonstrated superior performance in dyspnea score and PaCO compared to HFNC, helmet NIV, and COT. The length of stay in the hospital for face mask NIV was relatively longer compared to HFNC (WMD: -0.73, 95% CI: -1.35, -0.10) and COT (WMD: -1.09, 95% CI: -2.00, -0.18), and the probability of complications was higher than with HFNC. The rank probability suggested that COT had the lowest likelihood of intubation and all-cause mortality, while helmet NIV may have the best effect on improving respiratory rate.
Concerning treatment failure, dyspnea score, and PaCO improvement in patients with AHRF, face mask NIV may outperform other methods. For selected patients with AHRF, face mask NIV might be considered for potential first-line method. This study provides a certain level of evidence-based support for the management and treatment of AHRF, but more research is still needed in the future to determine the optimal non-invasive respiratory support method for treating patients with AHRF. In clinic, the efficacy of face mask NIV for better outcomes in patients with AHRH still requires validation.
本研究旨在比较不同的无创呼吸支持方法治疗急性高碳酸血症呼吸衰竭(AHRF)的效果。
基于PubMed、Embase、Cochrane图书馆和Web of Science数据库中从建库至2024年9月10日的研究进行网状Meta分析。结局指标为治疗失败、全因死亡率、气管插管、呼吸困难评分、住院时间、呼吸频率、动脉血二氧化碳分压(PaCO)及并发症。采用加权均数差或相对危险度及其各自的95%置信区间对直接和间接比较的结果进行定量评估,并以森林图进行图形化展示。此外,还给出了排序概率,表明每种无创呼吸支持方法在各项测量结局中最有效的可能性。
纳入19项研究(2022名参与者)。结果表明,面罩无创通气(NIV)治疗失败的概率低于高流量鼻导管吸氧(HFNC)(RR:1.42,95%CI:1.06,1.93)和传统氧疗(COT)(RR:1.87,95%CI:1.16,3.03)。与HFNC、头盔式NIV和COT相比,面罩NIV在呼吸困难评分和PaCO方面表现更优。与HFNC(WMD:-0.73,95%CI:-1.35,-0.10)和COT(WMD:-1.09,95%CI:-2.00,-0.18)相比,面罩NIV的住院时间相对较长,并发症发生概率高于HFNC。排序概率表明,COT气管插管和全因死亡率最低的可能性最大,而头盔式NIV可能对改善呼吸频率效果最佳。
在AHRF患者的治疗失败、呼吸困难评分及PaCO改善方面,面罩NIV可能优于其他方法。对于部分AHRF患者,可考虑将面罩NIV作为潜在的一线治疗方法。本研究为AHRF的管理和治疗提供了一定程度的循证支持,但未来仍需更多研究以确定治疗AHRF的最佳无创呼吸支持方法。在临床中,面罩NIV对AHRH患者取得更好结局的疗效仍需验证。