Kashyap Nishant, Subhash Abhijeet, Ahmed Wasim, Runu Ritesh, Kumar Santosh, Kumar Indrajeet
Orthopaedics, Indira Gandhi Institute of Medical Sciences, Patna, Patna, IND.
Cureus. 2025 Jun 25;17(6):e86766. doi: 10.7759/cureus.86766. eCollection 2025 Jun.
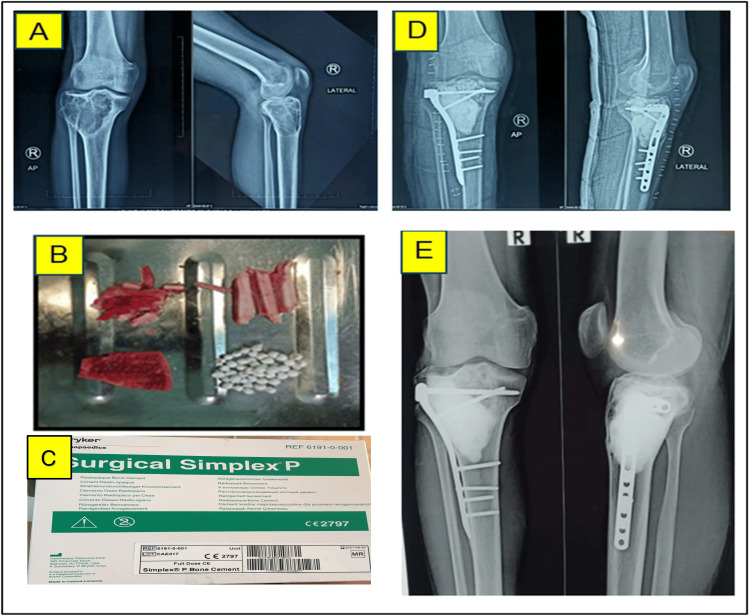
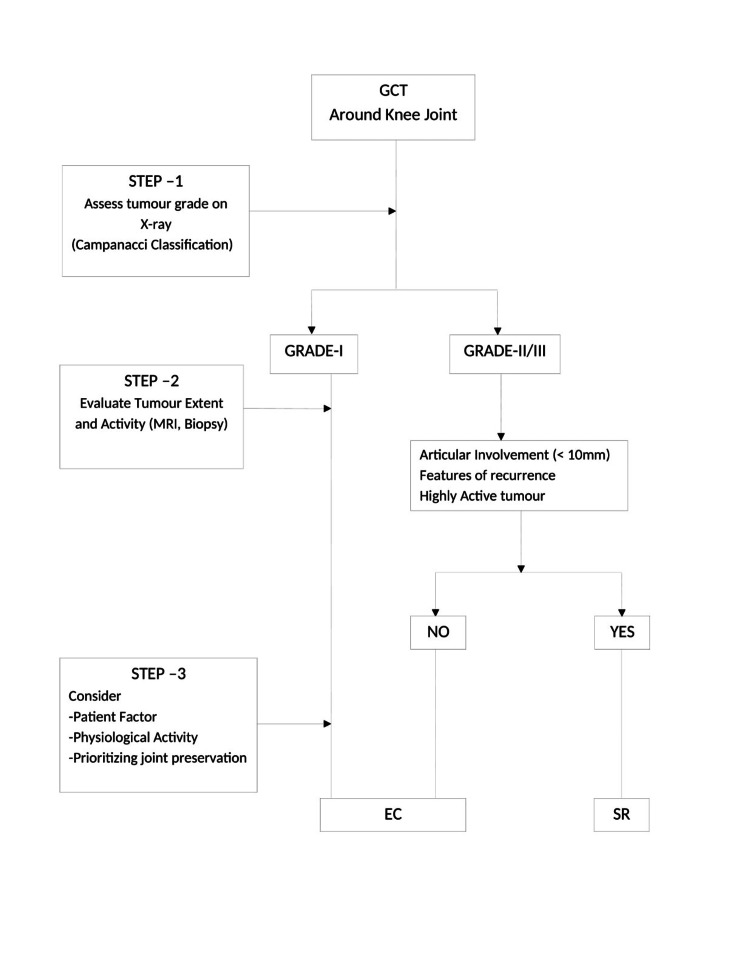
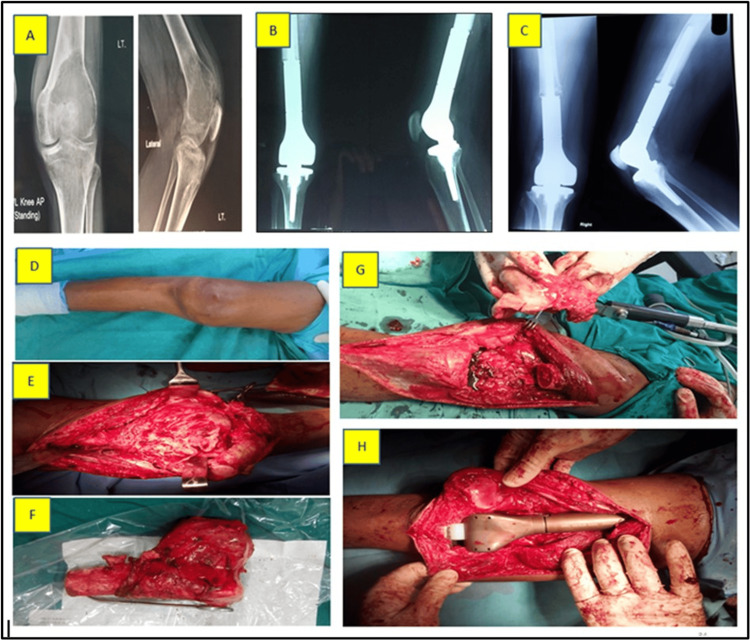
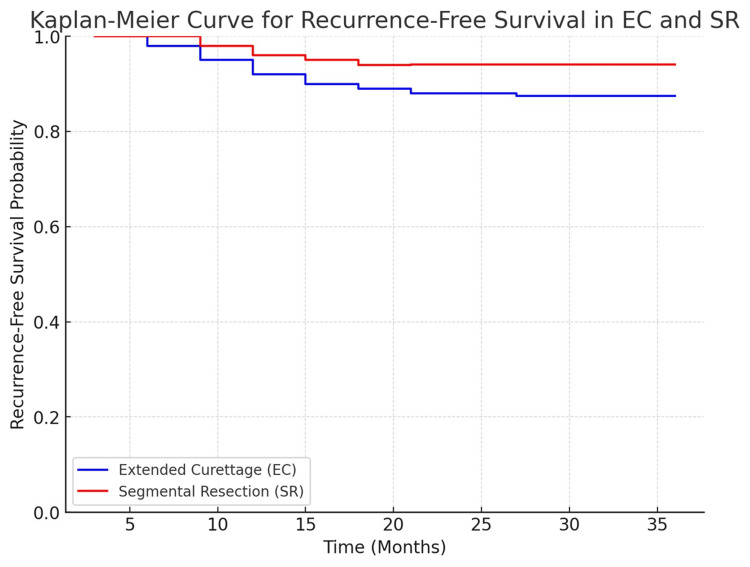
Background Giant cell tumors (GCTs) of bone around the knee are locally aggressive benign neoplasms with a tendency for recurrence and functional compromise. Surgical options include extended curettage (EC), often combined with adjuvants and internal fixation (sandwich technique), or segmental resection (SR) with megaprosthesis reconstruction. The optimal approach remains debated. This study compares oncological and functional outcomes between these two surgical strategies in a cohort of 65 patients. Methods A retrospective analysis was conducted at the Department of Orthopaedics, Indira Gandhi Institute of Medical Sciences, Patna, over six years. Patients with biopsy-confirmed GCTs around the knee who underwent EC or SR were included. Outcomes assessed included local recurrence, recurrence-free survival (RFS), Musculoskeletal Tumor Society (MSTS) scores, operative time, blood loss, hospital stay, and postoperative complications. Results Of the 65 patients (EC: 48; SR: 17), local recurrence was noted in 12.5% of the EC group and 5.9% of the SR group (p=0.762). For Grade II tumors, recurrence occurred in 4.2% of EC cases and none in SR; for Grade III tumors, recurrence rates were 8.3% (EC) and 5.9% (SR). At three years, RFS was 87.5% for EC and 94.1% for SR (p=0.604). SR involved longer surgeries (172.7 ± 36.3 vs. 119.2 ± 23.8 min, p<0.001), greater blood loss (656.8 ± 155.6 vs. 319.6 ± 127.9 mL, p<0.001), and longer hospital stays. EC demonstrated superior functional outcomes (MSTS: 25.5 ± 3.2 vs. 22.1 ± 3.8, p=0.007). Complication rates were higher in SR (35.3%) compared to EC (20.8%), though not statistically significant (p=0.268). Conclusion EC offers superior functional outcomes with a non-significant trend toward higher recurrence, whereas SR provides better local control at the cost of greater surgical morbidity. These findings suggest that patient selection should consider tumor grade, extent, and individual functional priorities. Prospective studies are needed to refine treatment algorithms and optimize outcomes.
膝关节周围的骨巨细胞瘤(GCTs)是具有局部侵袭性的良性肿瘤,有复发倾向且会导致功能受损。手术选择包括扩大刮除术(EC),通常联合辅助治疗及内固定(三明治技术),或采用带大假体重建的节段性切除术(SR)。最佳治疗方法仍存在争议。本研究比较了这两种手术策略在65例患者中的肿瘤学和功能结局。
在巴特那英迪拉·甘地医学科学研究所骨科进行了为期六年的回顾性分析。纳入经活检确诊为膝关节周围GCTs且接受了EC或SR的患者。评估的结局包括局部复发、无复发生存期(RFS)、肌肉骨骼肿瘤学会(MSTS)评分、手术时间、失血量、住院时间和术后并发症。
65例患者(EC组48例;SR组17例)中,EC组局部复发率为12.5%,SR组为5.9%(p = 0.762)。对于Ⅱ级肿瘤,EC组复发率为4.2%,SR组无复发;对于Ⅲ级肿瘤,EC组复发率为8.3%,SR组为5.9%。三年时,EC组的RFS为87.5%,SR组为94.1%(p = 0.604)。SR手术时间更长(172.7±36.3对119.2±23.8分钟,p<0.001),失血量更大(656.8±155.6对319.6±127.9毫升,p<0.001),住院时间更长。EC显示出更好的功能结局(MSTS评分:25.5±3.2对22.1±3.8,p = 0.007)。SR组的并发症发生率(35.3%)高于EC组(20.8%),但差异无统计学意义(p = 0.268)。
EC提供了更好的功能结局,复发率有升高趋势但不显著,而SR以更高的手术并发症为代价提供了更好的局部控制。这些发现表明,患者选择应考虑肿瘤分级、范围和个体功能优先事项。需要进行前瞻性研究以完善治疗方案并优化结局。