Jia Hang-Dong, Shi Zhe-Jin, Yuan Jian-Yong, Wang Kai, Yu Yang, Fang Zheng-Kang, Wang Kai-Di, Lu Yi, Shen Guo-Liang, Zhang Cheng-Wu, Liang Lei
General Surgery, Cancer Center, Department of Hepatobiliary & Pancreatic Surgery and Minimally Invasive Surgery, Affiliated People's Hospital, Zhejiang Provincial People's Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, China.
Department of Postgraduate Training, Base Alliance of Wenzhou Medical University, Wenzhou, Zhejiang, China.
Sci Rep. 2025 Jul 28;15(1):27407. doi: 10.1038/s41598-025-12400-0.
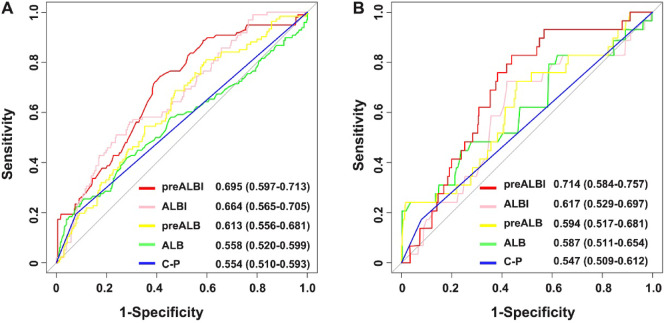
Post hepatectomy liver failure (PHLF) poses a significant threat to the prognosis of patients with hepatocellular carcinoma (HCC), particularly those undergoing major hepatectomy. The present research endeavors to clarify the influence of prealbumin on the development of PHLF in HCC patients who have undergone major hepatectomy. Patients with HCC who have undergone major hepatectomy were included. Based on the ROC curve, the optimal cut-off value for prealbumin was determined and patients were divided into two groups. Univariate and multivariate logistic analyses were conducted to identify risk factors for PHLF in HCC patients. Furthermore, the predictive ability of PHLF was also evaluated. 466 patients were included, among whom 98 (21%) developed PHLF. Compared with the high prealbumin group, patients in the low prealbumin group had significantly higher proportions of cirrhosis, portal hypertension, intraoperative blood loss, and transfusion, as well as a higher incidence of PHLF (12.3% vs. 23.5%, P = 0.011). Multivariate analysis revealed that prealbumin is a risk factor for PHLF (HR 1.446, 95%CI 1.091-2.369, P = 0.015), but it is not a risk factor for severe PHLF (HR 1.183, 95%CI 0.584-2.692, P = 0.289). However, the comprehensive indicator, prealbumin-bilirubin (preALBI), is not only a risk factor for PHLF but also severe PHLF. Furthermore, its predictive performance is significantly higher than that of other related indicators (all P < 0.05). Patients with low prealbumin levels require perioperative protocols: precise resection control, liver volume assessment, and PHLF prevention monitoring.
肝切除术后肝功能衰竭(PHLF)对肝细胞癌(HCC)患者的预后构成重大威胁,尤其是那些接受大肝切除术的患者。本研究旨在阐明前白蛋白对接受大肝切除术的HCC患者发生PHLF的影响。纳入接受大肝切除术的HCC患者。根据ROC曲线确定前白蛋白的最佳临界值,并将患者分为两组。进行单因素和多因素逻辑分析以确定HCC患者发生PHLF的危险因素。此外,还评估了PHLF的预测能力。共纳入466例患者,其中98例(21%)发生了PHLF。与前白蛋白水平高的组相比,前白蛋白水平低的组患者肝硬化、门静脉高压、术中失血和输血的比例显著更高,且PHLF的发生率也更高(12.3%对23.5%,P = 0.011)。多因素分析显示,前白蛋白是PHLF的危险因素(HR 1.446,95%CI 1.091 - 2.369,P = 0.015),但不是严重PHLF的危险因素(HR 1.183,95%CI 0.584 - 2.692,P = 0.289)。然而,综合指标前白蛋白-胆红素(preALBI)不仅是PHLF的危险因素,也是严重PHLF的危险因素。此外,其预测性能显著高于其他相关指标(所有P < 0.05)。前白蛋白水平低的患者需要围手术期方案:精确的切除控制、肝体积评估和PHLF预防监测。