Smith C A, Bögli S Y, Placek M M, Cabeleira M, White D, Daubney E, Young A, Beqiri E, Kayani R, O'Donnell R, Pathan N, Watson S, Maw A, Garnett M, Kanthimathinathan H K, Bangalore H, Sundararajan S, Subramanian G, Raffaj D, Lampariello S, Sarfatti A, Mayer A, Ross O, Czosnyka M, Hutchinson P J, Smielewski P, Agrawal S
Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK.
Department for Neurology and Neurocritical Care Unit, University Hospital and University of Zurich, Zurich, Switzerland.
EClinicalMedicine. 2025 Jul 17;86:103370. doi: 10.1016/j.eclinm.2025.103370. eCollection 2025 Aug.
Cerebral perfusion pressure (CPP) represents a key target for intensive care management of paediatric traumatic brain injury (TBI) patients. Current guidelines recommend a CPP target within the range of 40-50 mmHg but emphasise that these may depend on patient age and the state of cerebrovascular autoregulation. In this analysis, we aimed to compare the fixed targets proposed by the Brain Trauma Foundation to autoregulation-based targets CPPopt (optimal CPP) and LLA (Lower Limit of Autoregulation).
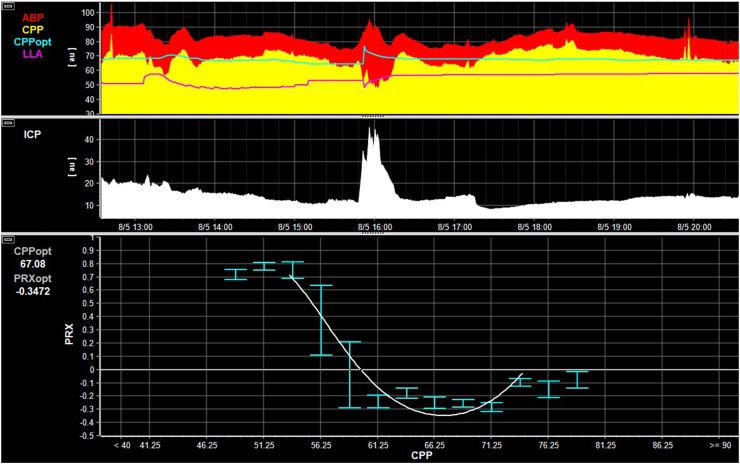
Data were acquired from the STARSHIP study (a prospective, multicentre, observational, research study which enrolled 135 children (median age 96 months (interquartile range 26-152 months)) with TBI between July 2018 and March 2023 across 10 paediatric intensive care units in the UK). In this secondary analysis the dose or percentage time spent below a fixed CPP target of 50 mmHg or CPPopt or LLA (assessed continuously on a minute-by-minute basis and derived by fitting a curve to the relationship between CPP and pressure reactivity index values, as previously described) was compared by outcome using univariable and multivariable methods. ClinicalTrials.gov registration-NCT0688462.
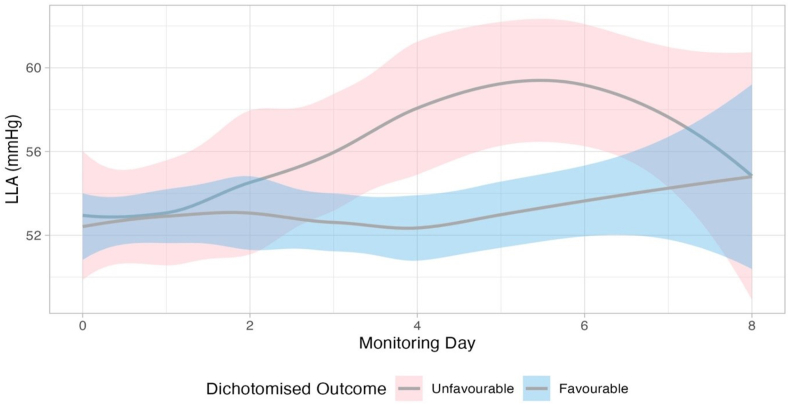
When assessed within ordinal analyses (to account for differences in baseline severity), both hourly dose and percentage time spent below LLA (odds ratio 1.01 [95% CI 1.00-1.02], p = 0.017 and 1.05 [95% CI 1.01-1.08], p = 0.008 respectively) were independently associated with worse outcomes. LLA displayed a dynamic time-trend increasing over time in patients with unfavourable outcome (n = 44, p = 0.003). Overall, LLA exceeded 50 mmHg for more than 45% of the monitoring period across all patients, and for over 35% of the time in the youngest cohort (0-2 years).
Dynamic autoregulation monitoring based on LLA was associated with outcomes in paediatric TBI with higher LLA values observed in individuals experiencing unfavourable outcomes. Our findings indicate that the current fixed CPP threshold of 40-50 mmHg may be too low-highlighting the need for further investigation into autoregulation-guided CPP targets. Whether personalised management based on autoregulatory-informed thresholds offers advantages over guideline-based targets remains to be determined and should be investigated in future prospective interventional studies.
Action Medical Research for Childrens' Charity and Addenbrookes Charitable Trust (UK Grant number-GN2609).
脑灌注压(CPP)是小儿创伤性脑损伤(TBI)患者重症监护管理的关键目标。当前指南推荐CPP目标范围为40 - 50 mmHg,但强调这些目标可能取决于患者年龄和脑血管自动调节状态。在本分析中,我们旨在比较脑创伤基金会提出的固定目标与基于自动调节的目标CPPopt(最佳CPP)和LLA(自动调节下限)。
数据来自STARSHIP研究(一项前瞻性、多中心、观察性研究,2018年7月至2023年3月期间在英国10个儿科重症监护病房招募了135名TBI儿童(中位年龄96个月(四分位间距26 - 152个月)))。在这项二次分析中,使用单变量和多变量方法按结局比较低于50 mmHg的固定CPP目标或CPPopt或LLA(如前所述,通过将曲线拟合到CPP与压力反应性指数值之间的关系逐分钟连续评估得出)的剂量或花费时间百分比。ClinicalTrials.gov注册号 - NCT0688462。
在序数分析中评估时(考虑基线严重程度差异),低于LLA的每小时剂量和花费时间百分比(优势比分别为1.01 [95% CI 1.00 - 1.02],p = 0.017和1.05 [95% CI 1.01 - 1.08],p = 0.008)均与更差的结局独立相关。LLA在预后不良的患者中随时间呈动态时间趋势增加(n = 44,p = 0.003)。总体而言,所有患者超过45%的监测期LLA超过50 mmHg,最年幼儿童队列(0 - 2岁)超过35%的时间如此。
基于LLA的动态自动调节监测与小儿TBI的结局相关,预后不良个体观察到更高的LLA值。我们的研究结果表明,当前40 - 50 mmHg的固定CPP阈值可能过低,凸显了对基于自动调节的CPP目标进行进一步研究的必要性。基于自动调节信息阈值的个性化管理是否优于基于指南的目标仍有待确定,应在未来的前瞻性干预研究中进行调查。
儿童慈善行动医学研究和阿登布鲁克慈善信托基金(英国资助编号 - GN2609)。