Wieske Viktoria, Walther Mario, Mohamed Mahmoud, Weickert Benjamin, Andrzejewski Simon, Dubourg Benjamin, Andreini Daniele, Pontone Gianluca, Alkadhi Hatem, Hausleiter Jörg, Garcia Mario J, Leschka Sebastian, Meijboom Willem B, Zimmermann Elke, Gerber Bernhard, Schoepf U Joseph, Shabestari Abbas A, Nørgaard Bjarne L, Meijs Matthijs Fl, Sato Akira, Øvrehus Kristian A, Diederichsen Axel Cp, Jenkins Shona M, Knuuti Juhani, Hamdan Ashraf, Halvorsen Bjørn A, Mendoza Rodriguez Vladimir, Rochitte Carlos, Rixe Johannes, Wan Yung-Liang, Langer Christoph, Bettencourt Nuno, Martuscelli Eugenio, Ghostine Said, Buechel Ronny R, Nikolaou Konstantin, Mickley Hans, Yang Lin, Zhang Zhaqoi, Chen Marcus Y, Halon David A, Rief Matthias, Sun Kai, Niinuma Hiroyuki, Marcus Roy P, Muraglia Simone, Jakamy Réda, Chow Benjamin Jw, Kaufmann Philipp A, Herzog Bernhard A, Tardif Jean-Claude, Nomura Cesar, Kofoed Klaus F, Laissy Jean-Pierre, Arbab-Zadeh Armin, Kitagawa Kakuya, Laham Roger, Jinzaki Masahiro, Hoe John, Rybicki Frank J, Scholte Arthur, Paul Narinder, Tan Swee Yaw, Yoshioka Kunihiro, Roehle Robert, Schuetz Georg M, Laule Michael, Newby David E, Achenbach Stephan, Budoff Matthew, Haase Robert, Dodd Jonathan D, Dewey Marc, Schlattmann Peter
Institute of Biometry and Clinical Epidemiology, Charité - Universitätsmedizin Berlin, Berlin, Germany.
Department of Fundamental Sciences, Jena University of Applied Sciences, Jena, Germany.
JACC Adv. 2025 Jul 28;4(8):102014. doi: 10.1016/j.jacadv.2025.102014.
Combining pretest probability (PTP) with computed tomography angiography (CTA) for diagnosing obstructive coronary artery disease (CAD) has not yet been determined.
The purpose of this study was to evaluate the accuracy of PTP calculation alone and with CTA for diagnosing CAD.
A total of 65 prospective diagnostic accuracy studies of patients clinically referred to invasive coronary angiography with stable chest pain were included in this international collaborative individual patient data Collaborative Meta-Analysis of Cardiac CT (COME-CCT) meta-analysis. Mixed-effects logistic regression with a data set-specific random intercept for clustering was applied to 4 models: the traditional Diamond-Forrester models, a PTP model based on the COME-CCT data (termed COME-CCT-PTP calculator), a CTA alone model, and a combined COME-CCT-PTP with CTA model.
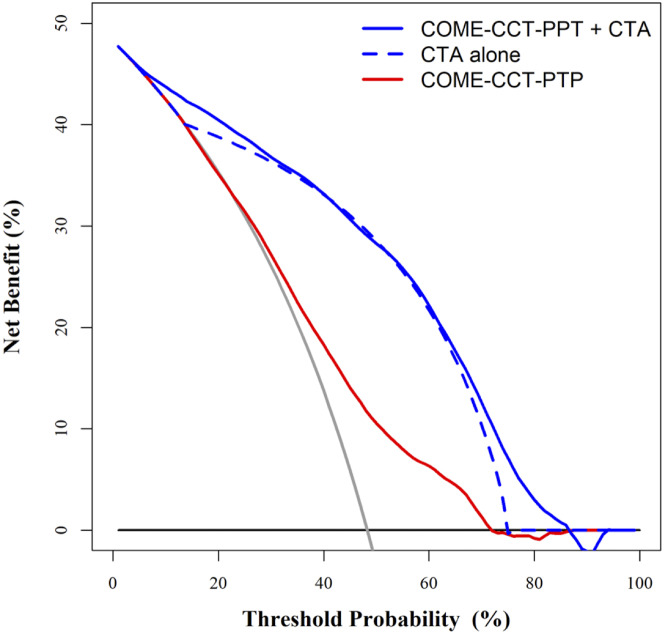
Individual patient data from 5,332 patients with clinically indicated invasive coronary angiography from 22 countries were included. The COME-CCT-PTP calculator was more accurate than the original Diamond-Forrester model (AUC: 0.68; 95% CI: 0.66-0.69 vs 0.63; 95% CI: 0.62-0.65). The COME-CCT-PTP with CTA model significantly improved accuracy compared with either model alone (AUC: 0.86; 95% CI: 0.85-0.87 vs 0.81; 95% CI: 0.80-0.82). The improved prediction was consistent in decision curve analysis with an increased net benefit for all chest pain subtypes and was almost equally seen in patients with typical or atypical angina (0.85; 95% CI: 0.84-0.86) and nonanginal or other chest discomfort (0.88; 95% CI: 0.86-0.89).
Combining the COME-CCT-PTP calculator with CTA provides more accurate prediction than the PTP or CTA alone for the diagnosis of obstructive CAD, for all chest pain subtypes.
尚未确定将预测试概率(PTP)与计算机断层扫描血管造影(CTA)相结合用于诊断阻塞性冠状动脉疾病(CAD)的情况。
本研究的目的是评估单独使用PTP计算以及联合CTA用于诊断CAD的准确性。
本国际合作个体患者数据心脏CT协作荟萃分析(COME-CCT)纳入了65项对临床转诊进行有创冠状动脉造影且有稳定胸痛症状患者的前瞻性诊断准确性研究。将具有特定数据集随机截距以进行聚类的混合效应逻辑回归应用于4个模型:传统的Diamond-Forrester模型、基于COME-CCT数据的PTP模型(称为COME-CCT-PTP计算器)、单独的CTA模型以及联合COME-CCT-PTP与CTA的模型。
纳入了来自22个国家的5332例临床指征进行有创冠状动脉造影患者的个体患者数据。COME-CCT-PTP计算器比原始的Diamond-Forrester模型更准确(曲线下面积[AUC]:0.68;95%置信区间[CI]:0.66 - 0.69对比0.63;95% CI:0.62 - 0.65)。与单独的任何一个模型相比,联合COME-CCT-PTP与CTA的模型显著提高了准确性(AUC:0.86;95% CI:0.85 - 0.87对比0.81;95% CI:0.80 - 0.82)。在决策曲线分析中,改进后的预测具有一致性,对所有胸痛亚型的净效益均增加,并且在典型或非典型心绞痛患者(0.85;95% CI:0.84 - 0.86)以及非心绞痛或其他胸部不适患者中几乎同样明显(0.88;95% CI:0.86 - 0.89)。
对于所有胸痛亚型,将COME-CCT-PTP计算器与CTA相结合用于诊断阻塞性CAD比单独使用PTP或CTA能提供更准确的预测。