Mangoni Arduino A, Wiese Michael D, Woodman Richard J, Sotgia Salvatore, Zinellu Angelo, Carru Ciriaco, Hulin Julie-Ann, Shanahan E Michael, Tommasi Sara
College of Medicine and Public Health, Flinders Health and Medical Research Institute, Flinders University, Adelaide, Australia.
Department of Clinical Pharmacology, Finders Medical Centre, Southern Adelaide Local Health Network, Adelaide, Australia.
Ann Med. 2025 Dec;57(1):2539311. doi: 10.1080/07853890.2025.2539311. Epub 2025 Jul 31.
Observational studies have shown that methotrexate, a conventional synthetic disease-modifying antirheumatic drug (csDMARD), is associated with lower arterial blood pressure (BP) and may reduce cardiovascular risk in rheumatoid arthritis (RA). However, it remains unclear whether a cause-and-effect relationship exists between the use of methotrexate and blood pressure reduction.
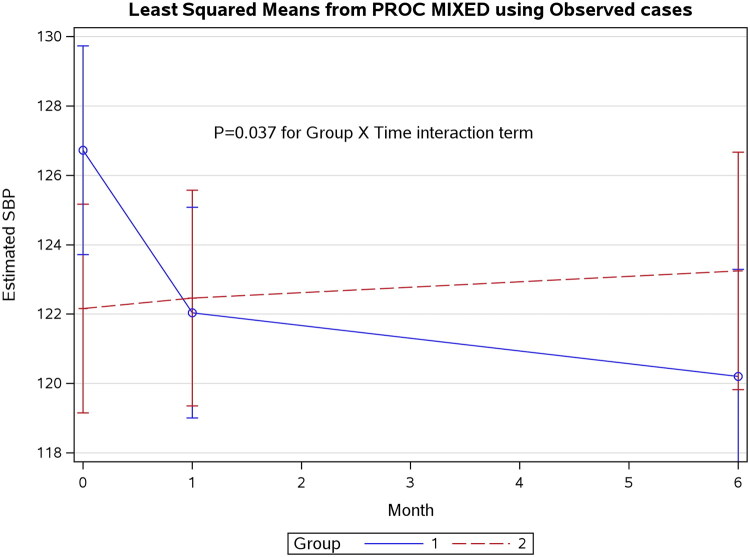
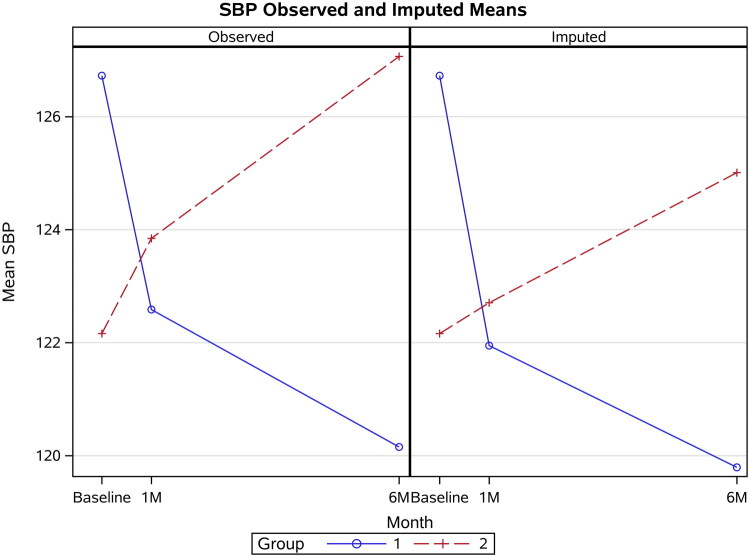
We conducted a controlled comparative study of treatment-naïve newly diagnosed RA patients commenced on subcutaneous methotrexate (Group 1, = 31, age 57 ± 15 years, 65% females, Disease Activity Score-28 - C-reactive protein, DAS28-CRP = 4.7 ± 1.2) or the DMARD comparator sulfasalazine (Group 2, = 31, 54 ± 17 years, 61% females, DAS28-CRP = 5.0 ± 0.8). Clinic systolic (SBP, primary study endpoint) and diastolic BP (DBP) and augmentation index (AIx, a marker of arterial stiffness) were measured at baseline and after one and six months of treatment (ClinicalTrials.gov: NCT03254589).
After six months, compared to Group 2, Group 1 patients had significantly lower SBP (-7.4 mmHg, 95% CI -14.0 to -0.8, = 0.03). By contrast, there were no significant between-group differences in DBP ( = 0.18), AIx ( = 0.85), or DAS28-CRP ( = 0.16). A significant effect of single nucleotide polymorphisms (SNPs) rs1801133 (methyl tetrahydrofolate reductase) and rs2231142 (ATP-binding cassette subfamily G member 2) on BP changes during methotrexate treatment was observed.
This is the first comparative study showing that methotrexate significantly reduces SBP in RA. This effect did not coincide with significant changes in arterial stiffness or disease activity. Further research is warranted to investigate the mechanisms underpinning the SBP-lowering effects of methotrexate, the role of specific SNPs, and whether such effects may account for reduced cardiovascular risk in patients with RA.
观察性研究表明,甲氨蝶呤作为一种传统的合成改善病情抗风湿药(csDMARD),与较低的动脉血压(BP)相关,并且可能降低类风湿关节炎(RA)患者的心血管风险。然而,甲氨蝶呤的使用与血压降低之间是否存在因果关系仍不清楚。
我们对初治的新诊断RA患者进行了一项对照比较研究,这些患者开始接受皮下注射甲氨蝶呤治疗(第1组,n = 31,年龄57±15岁,65%为女性,疾病活动评分-28 - C反应蛋白,DAS28-CRP = 4.7±1.2)或DMARD对照药物柳氮磺胺吡啶治疗(第2组,n = 31,54±17岁,61%为女性,DAS28-CRP = 5.0±0.8)。在基线以及治疗1个月和6个月后测量临床收缩压(SBP,主要研究终点)、舒张压(DBP)和增强指数(AIx,动脉僵硬度的标志物)(ClinicalTrials.gov:NCT03254589)。
6个月后,与第2组相比,第1组患者的SBP显著降低(-7.4 mmHg,95%CI -14.0至-0.8,P = 0.03)。相比之下,两组之间在DBP(P = 0.18)、AIx(P = 0.85)或DAS28-CRP(P = 0.16)方面没有显著差异。观察到单核苷酸多态性(SNP)rs1801133(甲基四氢叶酸还原酶)和rs2231142(ATP结合盒亚家族G成员2)对甲氨蝶呤治疗期间血压变化有显著影响。
这是第一项比较研究,表明甲氨蝶呤可显著降低RA患者的SBP。这种作用与动脉僵硬度或疾病活动度的显著变化不一致。有必要进一步研究以探讨甲氨蝶呤降低SBP作用的潜在机制、特定SNP的作用,以及这种作用是否可解释RA患者心血管风险的降低。