Kim Hae-Young, Eshun-Wilson Ingrid, Bridenbecker Daniel, Johnson Cheryl, Kisia Christine, Magare Jonah Onentiah, Geng Elvin H, Bershteyn Anna
New York University Grossman School of Medicine, New York City, New York, USA
Washington University in St Louis, St. Louis, Missouri, USA.
BMJ Open. 2025 Jul 30;15(7):e102999. doi: 10.1136/bmjopen-2025-102999.
To compare the impact of different HIV self-testing (HIVST) distribution modalities on population-level HIV outcomes.
Mathematical modelling study.
Six counties in western Kenya.
We projected population-level HIV outcomes among individuals aged 15+over 30 years (2022-2052) using EMOD-HIV, an agent-based network transmission model calibrated to the HIV epidemic in western Kenya. We simulated the impact of three HIVST distribution modalities: (1) secondary distribution to male partners via women who attend antenatal care visits ('ANC'); (2) secondary distribution to partners of individuals newly diagnosed with HIV at health facilities ('partner services'); and (3) distribution to any individuals attending outpatient clinics ('outpatient'). We informed our model assumptions on HIV testing uptake for each HIVST distribution modality using the estimates from a meta-analysis of randomised clinical trials published between 2006 and 2019 and compared the outcomes for each HIVST distribution modality to standard testing without HIVST.
The number of HIV tests performed (HIVST and non-HIVST), HIV diagnoses, HIV infections, and HIV-related deaths.
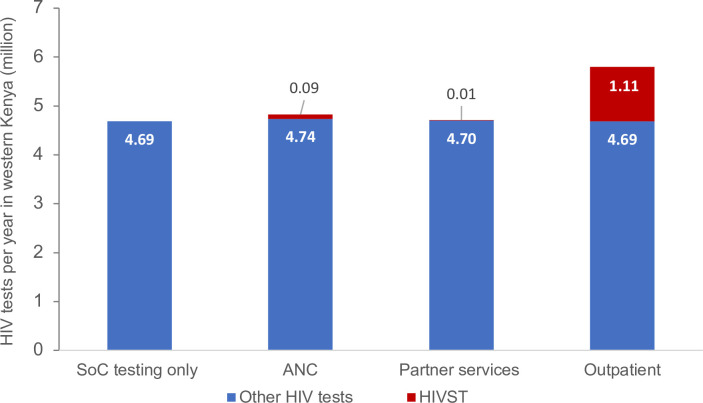
With standard testing alone, the average number of HIV tests was 4.69 million per year, amounting to 81.0 tests per 100 adults. The average number of tests per year increased by 2.9% with ANC, 0.6% with partner services, and 23.7% with outpatient distribution of HIVST. Compared with standard testing alone, partner services with HIVST will avert the largest number of new HIV infections (10.2%, 95% CI 9.9% to 10.5%), followed by outpatient distribution (8.5%, 95% CI 8.2% to 8.7%) and ANC (6.1%, 95% CI 5.8% to 6.3%). Compared with standard testing, the number of HIVST needed per one additional HIV infection averted was 216 with ANC, 17 with partner services and 2009 with outpatient, while the number of HIVST per one additional HIV-related death averted was 364 with ANC, 17 with partner services and 3851 with outpatient.
Secondary distribution of HIVST to partners of individuals newly diagnosed with HIV could prevent the most HIV infections and HIV-related deaths. HIVST can be an important strategy to improve uptake of testing and long-term population-level health effects.
比较不同的艾滋病毒自我检测(HIVST)分发方式对人群层面艾滋病毒相关结果的影响。
数学建模研究。
肯尼亚西部的六个县。
我们使用EMOD-HIV对15岁及以上人群在30年期间(2022 - 2052年)的人群层面艾滋病毒相关结果进行预测,EMOD-HIV是一个基于主体的网络传播模型,已根据肯尼亚西部的艾滋病毒疫情进行校准。我们模拟了三种HIVST分发方式的影响:(1)通过参加产前检查的女性向男性伴侣进行二次分发(“ANC”);(2)向在医疗机构新诊断出艾滋病毒的个人的伴侣进行二次分发(“伴侣服务”);(3)向任何前往门诊就诊的个人进行分发(“门诊”)。我们利用2006年至2019年发表的随机临床试验的荟萃分析估计值,为每种HIVST分发方式的艾滋病毒检测接受情况设定模型假设,并将每种HIVST分发方式的结果与无HIVST的标准检测结果进行比较。
进行的艾滋病毒检测数量(HIVST和非HIVST)、艾滋病毒诊断数、艾滋病毒感染数和与艾滋病毒相关的死亡数。
仅采用标准检测时,每年艾滋病毒检测的平均数量为469万次,相当于每100名成年人中有81.0次检测。采用ANC方式时,每年检测的平均数量增加了2.9%,采用伴侣服务方式时增加了0.6%,采用HIVST门诊分发方式时增加了23.7%。与仅采用标准检测相比,采用HIVST的伴侣服务方式将避免最多的新发艾滋病毒感染(10.2%,95%置信区间9.9%至10.5%),其次是门诊分发(8.5%,95%置信区间8.2%至8.7%)和ANC(6.1%,95%置信区间5.8%至6.3%)。与标准检测相比,采用ANC方式时,每避免一例额外的艾滋病毒感染所需的HIVST检测数量为216次,采用伴侣服务方式时为17次,采用门诊方式时为2009次;而采用ANC方式时,每避免一例额外的与艾滋病毒相关的死亡所需的HIVST检测数量为364次,采用伴侣服务方式时为17次,采用门诊方式时为3851次。
向新诊断出艾滋病毒的个人的伴侣进行HIVST二次分发可预防最多的艾滋病毒感染和与艾滋病毒相关的死亡。HIVST可以成为提高检测接受率和长期人群层面健康效果的重要策略。