Sakaguchi Masazumi, Tsunoda Shigeru, Nikaido Mitsuhiro, Teramoto Yuki, Okumura Shintaro, Hara Midori, Kitano Shoichi, Ueno Kohei, Aoyama Ryuhei, Yoshida Yu, Yamamoto Takehito, Sakamoto Takashi, Maeda Masahiro, Kasahara Keiko, Okamura Ryosuke, Hoshino Nobuaki, Itatani Yoshiro, Hisamori Shigeo, Hida Koya, Obama Kazutaka
Department of Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Kyoto, Japan.
Department of Gastroenterology, Tenri Hospital, Tenri, Nara, Japan.
Surg Case Rep. 2025;11(1). doi: 10.70352/scrj.cr.25-0346. Epub 2025 Jul 29.
Immunoglobulin G4-related disease (IgG4-RD) rarely involves the esophagus, typically causing stenosis that presents significant diagnostic and therapeutic challenges. Due to its rarity and its mimicry of other conditions, obtaining a definitive preoperative diagnosis can be difficult. This report details a case of IgG4-RD-induced esophageal stenosis with initial diagnostic ambiguity, which was successfully managed with mediastinoscopy-assisted esophagectomy (MAE), highlighting this minimally invasive approach in a patient with comorbidities.
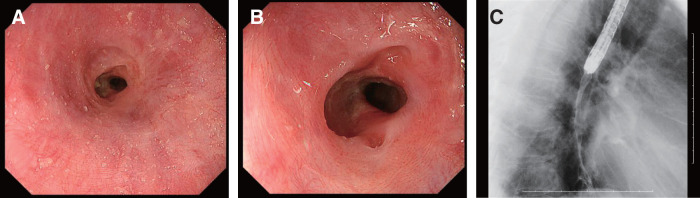
A 70-year-old male with comorbidities, including obstructive pulmonary disorder, presented with progressive dysphagia and epigastric discomfort. Endoscopy revealed a persistent mid-esophageal ulcer and a non-passable circumferential stricture; multiple biopsies were nondiagnostic for malignancy or infection. Given the refractory nature of the stenosis, MAE with gastric conduit reconstruction was performed. The postoperative course was uneventful, and the patient achieved symptom resolution without medication. Histopathological examination of the resected esophagus confirmed IgG4-RD, showing obliterative phlebitis and a dense infiltrate of IgG4-positive plasma cells (80/high-power field; IgG4/IgG ratio 80/85).
This case underscores that IgG4-RD should be considered in the differential diagnosis of refractory esophageal stenosis, even with initially inconclusive biopsies. While serum IgG4 measurement has low sensitivity, it is still recommended. For benign esophageal stenosis of unclear etiology, particularly in patients with significant comorbidities, MAE can be a useful and potentially curative surgical option, offering symptom resolution and the possibility of a drug-free outcome.
免疫球蛋白G4相关性疾病(IgG4-RD)很少累及食管,通常导致狭窄,这带来了重大的诊断和治疗挑战。由于其罕见性以及与其他疾病的相似性,术前获得明确诊断可能很困难。本报告详细介绍了一例IgG4-RD引起的食管狭窄病例,最初诊断存在模糊性,该病例通过纵隔镜辅助食管切除术(MAE)成功治疗,突出了这种微创方法在合并症患者中的应用。
一名70岁男性,患有包括阻塞性肺疾病在内的多种合并症,出现进行性吞咽困难和上腹部不适。内镜检查发现食管中段持续溃疡和不可通过的环形狭窄;多次活检未诊断出恶性肿瘤或感染。鉴于狭窄的难治性,进行了带胃管道重建的MAE。术后过程顺利,患者无需药物治疗症状即得到缓解。切除食管的组织病理学检查证实为IgG4-RD,显示闭塞性静脉炎和IgG4阳性浆细胞密集浸润(80/高倍视野;IgG4/IgG比例为80/85)。
该病例强调,即使最初活检结果不明确,在难治性食管狭窄的鉴别诊断中也应考虑IgG4-RD。虽然血清IgG4测量敏感性较低,但仍建议进行。对于病因不明的良性食管狭窄,特别是在合并症严重的患者中,MAE可能是一种有用且可能治愈的手术选择,可缓解症状并有可能实现无药物治疗的结果。