Ron Reut, Barnett Itzik, Berger Ruti, Sberro-Cohen Sarah
Assuta Health Services Research Institute, Tel-Aviv, Israel.
Ben-Gurion University of the Negev, Beer-Sheva, Israel.
BMC Nurs. 2025 Aug 5;24(1):1022. doi: 10.1186/s12912-025-03613-9.
Alarm fatigue in intensive care units (ICUs) is a pressing issue that jeopardizes patient safety and staff well-being. In Israel, although hospitals are permitted to determine who sets alarm thresholds, most have historically assigned this authority exclusively to physicians. This stems from the absence of national policy and institutional reluctance, driven by risk management and physician resistance to transfer clinical responsibilities to nurses, limiting timely responses to patient needs.
This was a prospective pre-post intervention study using multiple data sources, including structured observations and staff surveys, conducted in pediatric and adult general ICUs at Assuta Ashdod University Hospital. The intervention involved transferring alarm threshold-setting authority for bedside monitor alarms from physicians to nursing staff, supported by a comprehensive training program. Evaluation included structured observations of alarm events (435 pre- and 288 post-intervention), staff surveys (n = 33 pre, n = 24 post), and feedback on the implementation process.
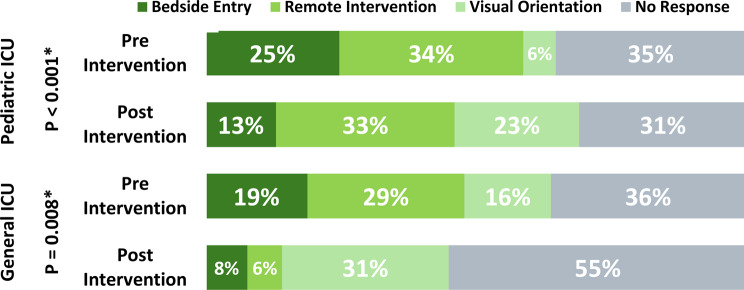
The primary outcome, alarm response rate-defined as the proportion of monitor alarms that elicited any observable staff reaction-increased slightly in the pediatric ICU, from 65 to 69%, and remained unchanged (50%) in the adult ICU. Notably, 90% of nurses in the pediatric ICU and 75% in the adult ICU reported increased confidence in setting alarm thresholds independently. Additionally, nursing staff expressed greater awareness of alarm fatigue and improved trust in alarm systems.
Empowering nursing staff by delegating alarm threshold authority resulted in enhanced alarm management and increased self-efficacy among nurses, though outcomes varied between units. These findings highlight the need for national guidelines to support this delegation while considering the unique characteristics of each ICU.
Not applicable.
重症监护病房(ICU)中的警报疲劳是一个紧迫的问题,危及患者安全和医护人员的健康。在以色列,尽管医院被允许决定由谁来设置警报阈值,但历史上大多数医院都将这项权力仅赋予医生。这源于缺乏国家政策以及机构的不情愿,风险管理和医生抵制将临床责任转交给护士导致了这种情况,限制了对患者需求的及时响应。
这是一项前瞻性干预前后研究,使用了多种数据源,包括结构化观察和员工调查,在阿苏塔阿什杜德大学医院的儿科和成人综合ICU中进行。干预措施包括将床边监护仪警报的阈值设置权从医生转移给护理人员,并辅以全面的培训计划。评估包括对警报事件的结构化观察(干预前435次,干预后288次)、员工调查(干预前n = 33,干预后n = 24)以及对实施过程的反馈。
主要结果是警报响应率,定义为引发任何可观察到的员工反应的监护仪警报比例。在儿科ICU中略有增加,从65%增至69%,在成人ICU中保持不变(50%)。值得注意的是,儿科ICU中90%的护士和成人ICU中75%的护士报告称独立设置警报阈值的信心增强。此外,护理人员对警报疲劳的认识提高,对警报系统的信任增强。
通过下放警报阈值设置权赋予护理人员权力,虽各科室结果有所不同,但增强了警报管理并提高了护士的自我效能感。这些发现凸显了需要国家指南来支持这种权力下放,同时考虑每个ICU的独特特征。
不适用。