Reizine Florian, Stiegler Vicky, Lécuyer Romain, Tessoulin Benoit, Gallais Marie, Camou Fabrice, Morio Florent, Cady Anne, Gabriel Frederic, Canet Emmanuel, Raffi François, Boutoille David, Issa Nahéma, Gaborit Benjamin
Service de Réanimation Polyvalente, Centre Hospitalier Bretagne-Atlantique, 56000, Vannes, France.
Department of Infectious Diseases, INSERM, University Hospital of Nantes and Centre d'Investigation Clinique 1413, Nantes, France.
Ann Intensive Care. 2025 Aug 6;15(1):114. doi: 10.1186/s13613-025-01503-6.
Pneumocystis jirovecii pneumonia (PjP) is a rising cause of acute respiratory failure in immunocompromised patients, often requiring Intensive Care Unit (ICU) admission. However, optimal ventilatory strategies remain unclear.
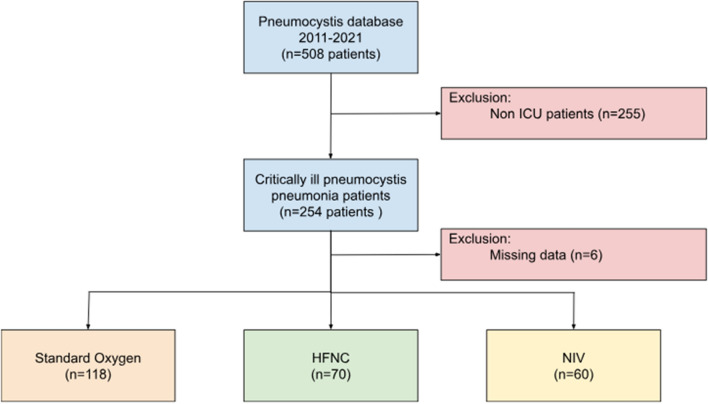
For the present study, we conducted an ancillary analysis of the PRONOCYSTIS study, a large multicenter cohort of PjP patients. Patients admitted to the ICUs were compared according to initial respiratory management (High-Flow Nasal Cannula (HFNC), standard Oxygen (SO) or Non-Invasive Ventilation (NIV). A propensity score adjustment [inverse probability of treatment weighting (IPTW) analysis] was implemented to account for potential confounders. The primary outcome was intubation rate. Univariable and multivariable Cox regressions were also used to assess variables associated with survival.
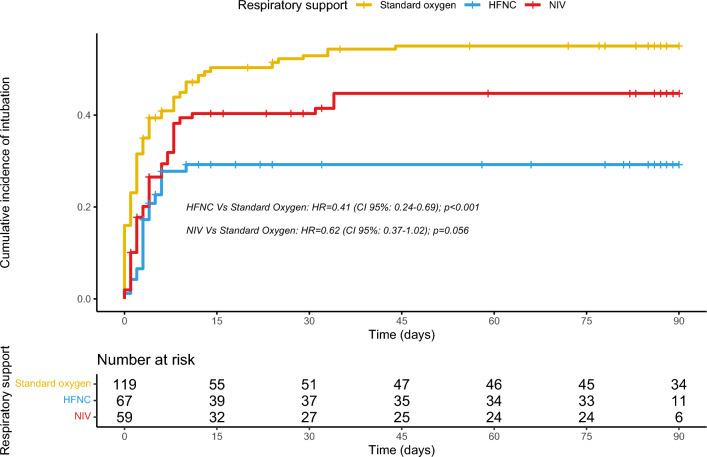
Over the study period, 248 patients with PjP were included in the present analysis. Of those, 70 were treated by HFNC while 118 and 60 received SO and NIV, respectively. HFNC patients had a decreased intubation rate (28.6% versus 45.0% in NIV and 55.4% in SO patients; p = 0.003). When assessing the impact of respiratory management on intubation by IPTW, HFNC remained an independent protective factor (weighted Hazard Ratio (HR) 0.41 (95% CI 0.24-0.69); p < 0.001). While, NIV was not associated with intubation (HR 0.62 (95% CI 0.37-1.02); p = 0.056). Through adjusted survival analysis, long-term corticosteroids treatment (aHR 4.03 (95% CI 2.01-8.08); p < 0.001), Solid tumor (aHR 3.37 (95% CI 1.45-7.86); p = 0.005) and the Sequential Organ Failure Assessment score (aHR 1.24 (95% CI 1.15-1.35); p < 0.001) were found to be independent predictor for death. Initial respiratory support was not associated with survival either in the Cox multivariable analysis or in the IPTW analysis.
Through this multicenter observational study of severe PjP patients, although oxygenation strategy was not associated with D90 survival, HFNC support appeared to be associated with a lower intubation rate. Further prospective studies are warranted to refine respiratory management in critically ill PjP patients.
耶氏肺孢子菌肺炎(PjP)是免疫功能低下患者急性呼吸衰竭的一个日益常见的病因,这类患者常需入住重症监护病房(ICU)。然而,最佳通气策略仍不明确。
在本研究中,我们对PRONOCYSTIS研究进行了一项辅助分析,该研究是一个关于PjP患者的大型多中心队列研究。根据初始呼吸管理方式(高流量鼻导管吸氧(HFNC)、标准吸氧(SO)或无创通气(NIV))对入住ICU的患者进行比较。采用倾向评分调整[治疗权重逆概率(IPTW)分析]来处理潜在的混杂因素。主要结局是插管率。还使用单变量和多变量Cox回归来评估与生存相关的变量。
在研究期间,本分析纳入了248例PjP患者。其中,70例接受HFNC治疗,118例和60例分别接受SO和NIV治疗。HFNC组患者的插管率降低(NIV组为45.0%,SO组为55.4%,HFNC组为28.6%;p = 0.003)。通过IPTW评估呼吸管理对插管的影响时,HFNC仍然是一个独立的保护因素(加权风险比(HR)0.41(95%CI 0.24 - 0.69);p < 0.001)。而NIV与插管无关(HR 0.62(95%CI 0.37 - 1.02);p = 0.056)。通过校正生存分析,长期使用皮质类固醇治疗(校正后HR 4.03(95%CI 2.01 - 8.08);p < 0.001)、实体瘤(校正后HR 3.37(95%CI 1.45 - 7.86);p = 0.005)和序贯器官衰竭评估评分(校正后HR 1.24(95%CI 1.15 - 1.35);p < 0.001)被发现是死亡的独立预测因素。在Cox多变量分析或IPTW分析中,初始呼吸支持与生存均无关。
通过这项对重症PjP患者的多中心观察性研究,虽然氧合策略与90天生存率无关,但HFNC支持似乎与较低的插管率相关。有必要进行进一步的前瞻性研究,以优化重症PjP患者的呼吸管理。