Aujla Usman I, Malik Ahmad Karim, Saeed Abdullah, Rafi Kashif, Syed Imran Ali
Gastroenterology and Hepatology, Pakistan Kidney and Liver Institute and Research Center, Lahore, PAK.
Radiology, Pakistan Kidney and Liver Institute and Research Center, Lahore, PAK.
Cureus. 2025 Jul 7;17(7):e87427. doi: 10.7759/cureus.87427. eCollection 2025 Jul.
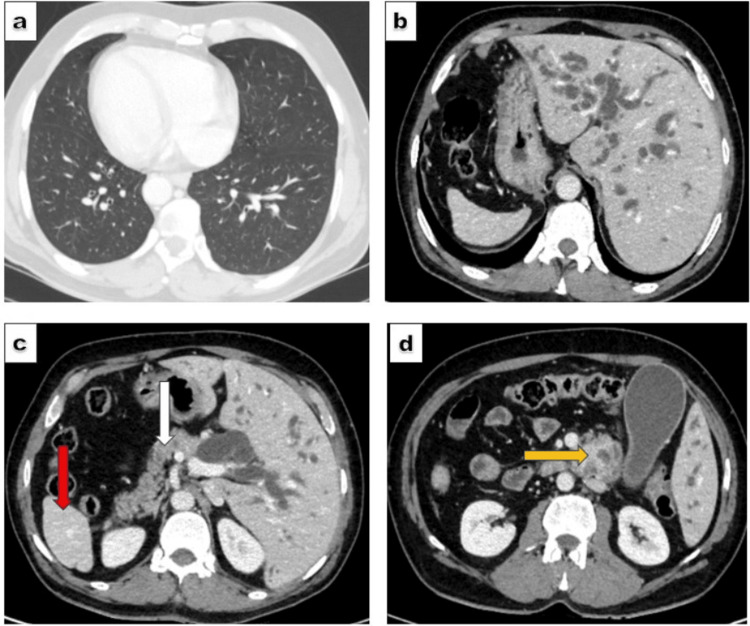
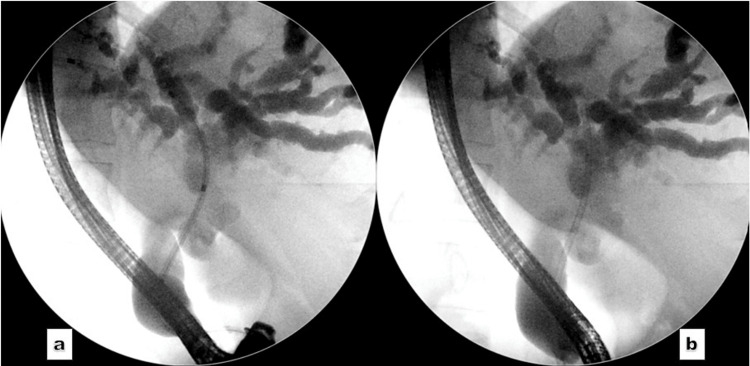
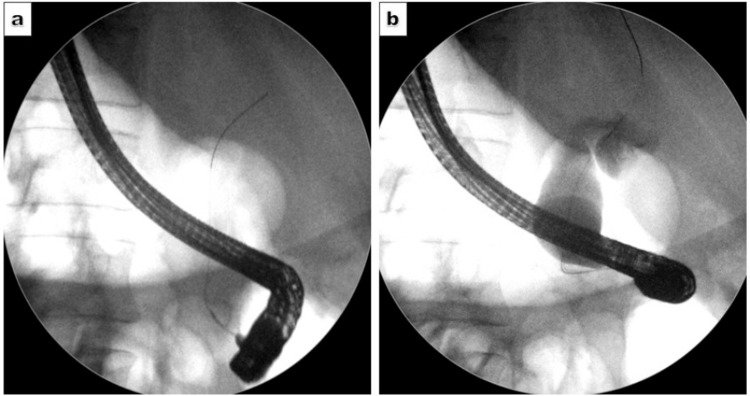
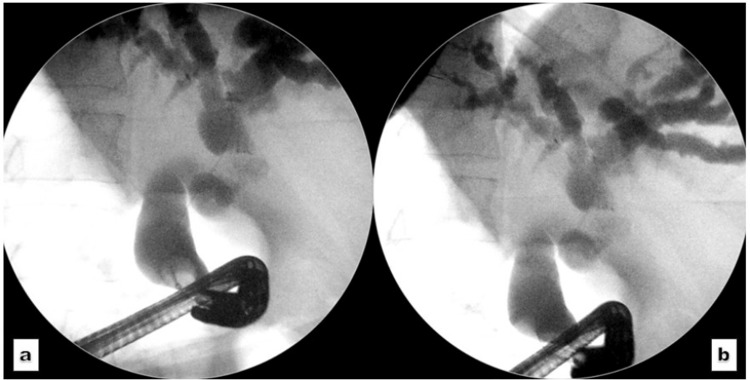
Situs inversus totalis (SIT) is a rare condition characterised by the reversed positioning of abdominal and thoracic viscera. The anomaly poses a significant anatomical challenge during routine endoscopic procedures, including endoscopic retrograde cholangiopancreatography (ERCP). Here, we present the case of a 51-year-old patient with SIT and obstructive jaundice due to a periampullary mass. Initial ERCP attempts at an external facility for biliary decompression were unsuccessful, prompting referral to our center. Multidisciplinary consensus recommended preoperative ERCP followed by a Whipple's procedure. ERCP was performed with positional adjustments (prone position) of the patient and significant scope manipulation (stepwise 360-degree anticlockwise rotation) to navigate the reversed anatomy. Cannulation was achieved, and a plastic biliary stent was placed, resulting in effective drainage. The patient demonstrated clinical improvement and was referred for surgical intervention. A comprehensive understanding of the reversed anatomy, along with the operator's skill and experience, is essential to address the challenges posed by this unique anatomical variation.
全内脏反位(SIT)是一种罕见的病症,其特征为腹部和胸部脏器位置颠倒。在包括内镜逆行胰胆管造影术(ERCP)在内的常规内镜检查过程中,这种异常情况会带来重大的解剖学挑战。在此,我们报告一例51岁患有SIT且因壶腹周围肿块导致梗阻性黄疸的患者。在外部机构最初尝试进行ERCP以实现胆道减压未成功,促使患者转诊至我们中心。多学科共识建议先进行术前ERCP,然后施行惠普尔手术。通过调整患者体位(俯卧位)并进行大幅度的内镜操作(360度逆时针逐步旋转)来应对解剖结构倒置的情况,从而完成了ERCP。成功实现插管,并置入了塑料胆道支架,实现了有效引流。患者临床症状改善,并被转诊接受手术干预。全面了解解剖结构的倒置情况,以及操作者的技能和经验,对于应对这种独特解剖变异所带来的挑战至关重要。