Stone H H, Fulenwider J T
Ann Surg. 1977 Sep;186(3):343-55. doi: 10.1097/00000658-197709000-00012.
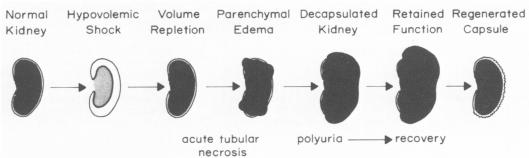
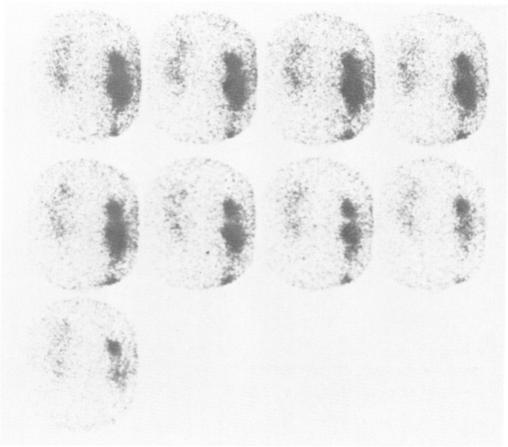
The delayed onset of anuria/oliguria in acute tubular necrosis has been theorized to represent a complicating compartment syndrome, i.e., parenchymal swelling within an unyielding capsule. To test this proposition, 12 monkeys had suprarenal aortic cross-clamping, followed by unilateral renal decapsulation to create an experimental as well as a control kidney unit in the same animal. Histologic examination uniformly confirmed tubular necrosis at death or sacrifice. Subsequent split renal function studies (creatinine, urea, and free water clearances) indicated significantly greater maintenance of renal function by the decapsulated kidney than by its paired control. Clinical evaluation in 21 hemorrhagic shock patients, with the capsule of one kidney stripped, revealed on follow-up that 15 developed a renal failure consistent with acute tubular necrosis. Although three patients with polyuric failure died before split studies could be run and two others have been too recent for computer analysis to have been completed, nine of the remaining ten had significantly greater renal plasma flows (194 versus 121 ml/min M(2), p < .01) and significantly greater urine flows (.99 versus .18 ml/min M(2), p < .01) on the decapsulated side than on the control, as determined by differential renal scans. No significant difference in these same lateralized renal functions was noted in the tenth patient with renal failure and in the six survivors without renal failure. Renal decapsulation as prophylaxis reduced the anticipated incidence of oliguria/anuria from an expected 75% to 7% (p < .01) in these 21 shock patients. Such data suggest that delayed renal ischemia, possibly based on a compartment syndrome, may be the cause for a progression of acute tubular necrosis from polyuria to oliguria and then to anuria.
急性肾小管坏死中无尿/少尿的延迟发作被认为代表一种并发的间隔综合征,即坚硬包膜内的实质肿胀。为验证这一观点,对12只猴子进行了肾上主动脉交叉钳夹,随后进行单侧肾被膜剥除,在同一只动物体内创建了一个实验性肾单位和一个对照肾单位。组织学检查一致证实死亡或处死后存在肾小管坏死。随后的分侧肾功能研究(肌酐、尿素和自由水清除率)表明,被膜剥除的肾脏比其配对的对照肾脏在肾功能维持方面显著更好。对21例失血性休克患者进行临床评估,其中一侧肾脏被膜剥除,随访发现15例发生了与急性肾小管坏死一致的肾衰竭。尽管3例多尿性肾衰竭患者在分侧研究能够进行之前死亡,另外2例因时间过近计算机分析尚未完成,但其余10例中的9例,经分侧肾扫描测定,被膜剥除侧的肾血浆流量(平均每平方米体表面积194对121毫升/分钟,p<0.01)和尿流量(平均每平方米体表面积0.99对0.18毫升/分钟,p<0.01)显著高于对照侧。在第10例肾衰竭患者和6例无肾衰竭的幸存者中,这些分侧肾功能无显著差异。在这21例休克患者中,预防性肾被膜剥除使少尿/无尿的预期发生率从预期的75%降至7%(p<0.01)。这些数据表明,可能基于间隔综合征的延迟性肾缺血可能是急性肾小管坏死从多尿发展为少尿进而发展为无尿的原因。