Ishigami Junichi, Surapaneni Aditya, Matsushita Kunihiro, Coresh Josef, Grams Morgan E, Ballew Shoshana H, Sang Yingying, Stengel Benedicte, Ärnlöv Johan, Bell Samira, Carrero Juan-Jesus, Chang Alexander R, Ciemins Elizabeth L, Haynes Richard, Ix Joachim, Kotsis Fruzsina, Lees Jennifer S, Pandit Krutika, Rao Panduranga, Robinson-Cohen Cassianne, Alencar de Pinho Natalia, Sumida Keiichi
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Welch Center for Prevention, Epidemiology, and Clinical Research, Johns Hopkins University, Baltimore, MD, USA.
EClinicalMedicine. 2025 Jul 31;86:103372. doi: 10.1016/j.eclinm.2025.103372. eCollection 2025 Aug.
Infections are a major cause of hospitalization in people with chronic kidney disease (CKD), with incidence similar to cardiovascular disease, yet the risk of infection has not been systematically studied across stages of CKD.
We conducted a meta-analysis of individual participant data including 1,246,912 individuals across 47 cohorts in the CKD Prognosis Consortium, with information on estimated glomerular filtration rate based on serum creatinine (eGFRcr) and urinary albuminuria (ACR) (or proteinuria converted to ACR), to examine the association of eGFR and ACR with the risk of hospitalization with infection. Outcomes were ascertained through diagnostic codes on hospital discharge records relevant to acute infections (i.e., upper and lower respiratory tract, urinary tract, skin and soft tissue, musculoskeletal, gastrointestinal tract, genital, nervous system, and cardiovascular system infections, and sepsis). Follow-up was censored on December 31, 2019 or on the last date of cohort follow-up, whichever was earlier. Multivariable Cox models were used to estimate hazard ratios (HRs).
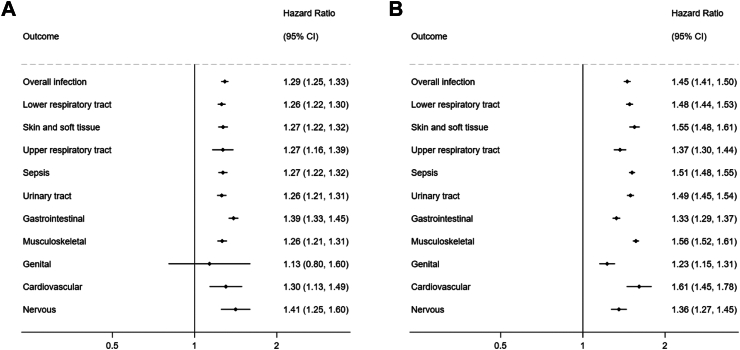
During follow-up, 170,864 (13.7%) individuals had a hospitalization with infection (IR, 22.0 [IQI, 16.2-31.0] per 1000 person-yrs). In Cox models, compared to eGFRcr 90-104 ml/min/1.73 m and ACR <10 mg/g, lower eGFRcr and higher ACR were each independently associated with an increased hazard of infection in a graded manner, including in eGFRcr 60-89 and 45-59 ml/min/1.73 m (adjusted HRs [95% CI], 1.09 [1.06-1.13] and 1.39 [1.34-1.45]) and ACR 10-29 and 30-299 mg/g (1.40 [1.33-1.47] and 1.82 [1.72-1.92]). High eGFRcr ≥105 ml/min/1.73 m was also associated with the risk of infection (1.22 [1.17-1.26]). Combined, eGFRcr <30 ml/min/1.73 m and ACR ≥ 300 mg/g were associated with more than 6-fold higher hazard of infections (6.27 [5.70-6.90]). These findings were consistent across infection subtypes (e.g., HRs for lower respiratory tract infections, 1.26 [1.22-1.30] per -15 ml/min/1.73 m in eGFR and 1.48 [1.44-1.53] per 8-fold increase in ACR).
Lower kidney function and higher albuminuria were independently associated with higher risk of infection. The risk was elevated even in mild to moderate CKD, with the highest risk seen in the most advanced stage of CKD. Infection prevention measures should target individuals across all CKD stages.
US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases.
感染是慢性肾脏病(CKD)患者住院的主要原因,其发病率与心血管疾病相似,但尚未对CKD各阶段的感染风险进行系统研究。
我们对慢性肾脏病预后协作组中47个队列的1,246,912名个体的个体参与者数据进行了荟萃分析,这些数据包含基于血清肌酐的估计肾小球滤过率(eGFRcr)和尿白蛋白尿(ACR)(或转换为ACR的蛋白尿)信息,以研究eGFR和ACR与感染住院风险之间的关联。通过医院出院记录上与急性感染相关的诊断代码(即上、下呼吸道、泌尿道、皮肤和软组织、肌肉骨骼、胃肠道、生殖器、神经系统和心血管系统感染以及败血症)确定结局。随访于2019年12月31日或队列随访的最后日期(以较早者为准)进行截尾。使用多变量Cox模型估计风险比(HRs)。
在随访期间,170,864名(13.7%)个体因感染住院(发病率,每1000人年22.0[四分位间距,16.2 - 31.0])。在Cox模型中,与eGFRcr 90 - 104 ml/min/1.73 m和ACR <10 mg/g相比,较低的eGFRcr和较高的ACR均以分级方式独立与感染风险增加相关,包括eGFRcr 60 - 89和45 - 59 ml/min/1.73 m(校正HRs[95%CI],1.09[1.06 - 1.13]和1.39[1.34 - 1.45])以及ACR 10 - 29和30 - 299 mg/g(1.40[1.33 - 1.47]和1.82[1.72 - 1.92])。高eGFRcr≥105 ml/min/1.73 m也与感染风险相关(1.22[1.17 - 1.26])。综合来看,eGFRcr <30 ml/min/1.73 m和ACR≥300 mg/g与感染风险高出6倍以上相关(6.27[5.70 - 6.90])。这些发现 across infection subtypes(例如,下呼吸道感染的HRs,eGFR每降低15 ml/min/1.73 m为(1.26[1.22 - 1.30]),ACR每增加8倍为(1.48[1.44 - 1.53]))。
较低的肾功能和较高的白蛋白尿与较高的感染风险独立相关。即使在轻度至中度CKD中风险也会升高,在CKD最晚期风险最高。感染预防措施应针对所有CKD阶段的个体。
美国国家肾脏基金会以及美国国立糖尿病、消化和肾脏疾病研究所。