Zhang Hao-Ting, Liu Fang-Jie, Wang Da-Quan, Xiong Yi-Xin, Zhao Yuan-Yuan, He Wen-Zhuo, Zhang Peng-Xin, Zheng Shi-Yang, Xia Biao, Situ Yu, Wang Meng-Ru, Liu Qian-Wen, Hu Yi, Xia Liang-Ping, Qiu Bo, Liu Hui
Department of Radiation Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangdong Provincial Clinical Research Center for Cancer, Guangzhou, China.
Guangdong University of Foreign Studies School of Economics and Trade, Guangzhou Higher Education Mega Center, Guangzhou, China.
Transl Lung Cancer Res. 2025 Jul 31;14(7):2710-2722. doi: 10.21037/tlcr-2025-190. Epub 2025 Jul 28.
Concurrent chemoradiotherapy (CCRT) followed by consolidative immunotherapy represents the standard of care for unresectable locally advanced non-small cell lung cancer (LA-NSCLC), but critical challenges persist: a considerable number of patients discontinue consolidative immune checkpoint inhibitors (ICIs) due to treatment-related pneumonitis and lymphopenia, while "cold" tumor microenvironments further limit immunotherapy efficacy. Thymosin α1 (Tα1) is a pleiotropic immunomodulator that has been associated with infection prevention and the regulation of immune cells. Thus, we designed this retrospective study to investigate the therapeutic effect of integrating Tα1 into CCRT followed by consolidative immunotherapy in patients diagnosed with unresectable LA-NSCLC.
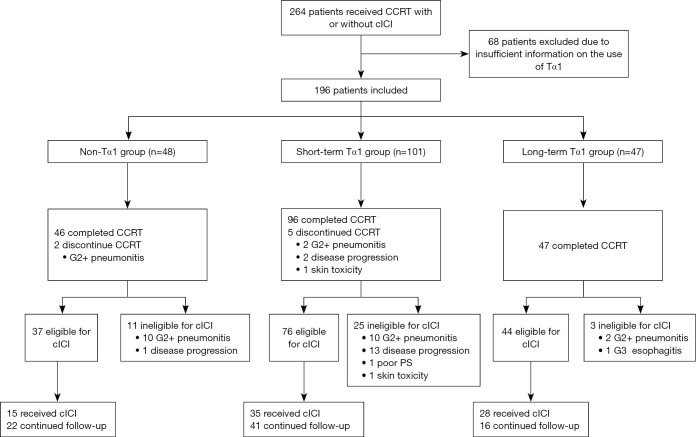
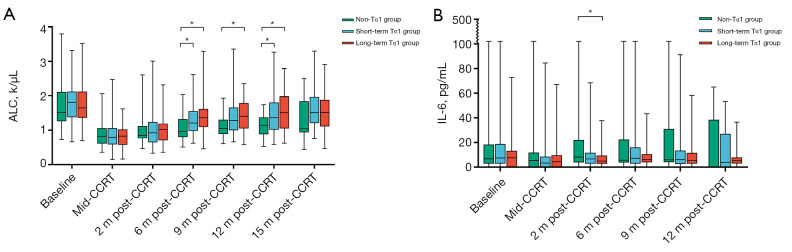
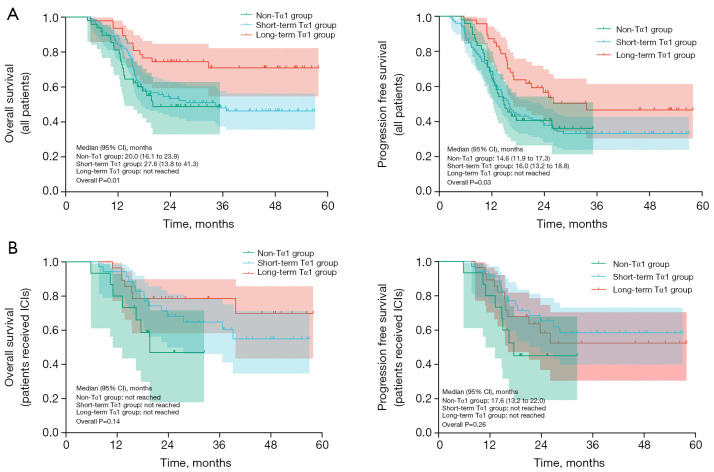
A retrospective analysis was conducted on a total of 196 patients with unresectable stage IIIA-IIIC LA-NSCLC treated from January 1, 2020, to May 31, 2023. All patients received CCRT (60-64 Gy total irradiation dose, weekly concurrent docetaxel and cisplatin) with or without consolidative nivolumab. According to the use of Tα1, patients were classified into 3 groups: non-Tα1 group, patients who did not receive Tα1; short-term Tα1 group, receipt of Tα1 (1.6 mg) once a week from the beginning of treatment until the end of CCRT; long-term Tα1 group, receipt of Tα1 (1.6 mg) once a week from the beginning of treatment until 12 months post-CCRT. The primary objective was progression-free survival (PFS). The secondary objectives included overall survival (OS), pneumonitis, circulating lymphocyte count and interleukin-6 (IL-6) levels. Pretreatment biopsy samples were collected to evaluate the potential influence of somatic mutations on treatment outcomes.
The non-Tα1, short-term Tα1, and long-term Tα1 groups included 48, 101, and 47 patients, respectively. Following CCRT, 77.1%, 75.2%, and 93.6% of patients in the respective groups were eligible for consolidative nivolumab (P=0.03). Median PFS was 14.6 months [95% confidence interval (CI): 11.9-17.3] for the non-Tα1 group, 16.0 months (95% CI: 13.2-18.8) for the short-term Tα1 group, and not reached for the long-term Tα1 group (P=0.03). Median OS was 20.0 months (95% CI: 16.1-23.9) for the non-Tα1 group, 27.6 months (95% CI: 13.8-41.3) for the short-term Tα1 group, and not reached in the long-term Tα1 group (P=0.01). The long-term Tα1 group experienced significantly lower rates of grade ≥2 pneumonitis (35.4% in non-Tα1, 14.5% in long-term Tα1 groups, P=0.02), and lower rates of lymphopenia at 6 months post-CCRT (55.8% in non-Tα1, 30.9% in short-term Tα1, and 22.5% in long-term Tα1 groups, P=0.01). At 2 months post-CCRT, the median IL-6 level in the non-Tα1 group (8.14 pg/mL) was significantly higher than that in the long-term Tα1 group (4.92 pg/mL, P=0.03).
Integrating Tα1 into CCRT and consolidative immunotherapy could have a synergistic effect in patients with LA-NSCLC. This combination may enhance survival outcomes and reduce treatment-related toxicity. Further randomized trial is warranted for validation.
同步放化疗(CCRT)后进行巩固性免疫治疗是不可切除的局部晚期非小细胞肺癌(LA-NSCLC)的标准治疗方案,但仍存在重大挑战:相当数量的患者因治疗相关的肺炎和淋巴细胞减少而中断巩固性免疫检查点抑制剂(ICI)治疗,而“冷”肿瘤微环境进一步限制了免疫治疗的疗效。胸腺肽α1(Tα1)是一种多效性免疫调节剂,与预防感染和免疫细胞调节有关。因此,我们设计了这项回顾性研究,以探讨在诊断为不可切除的LA-NSCLC患者中,将Tα1纳入CCRT后进行巩固性免疫治疗的疗效。
对2020年1月1日至2023年5月31日期间治疗的196例不可切除的IIIA-IIIC期LA-NSCLC患者进行回顾性分析。所有患者均接受CCRT(总照射剂量60-64 Gy,每周同步多西他赛和顺铂),部分患者接受或不接受巩固性纳武单抗治疗。根据Tα1的使用情况,患者分为3组:非Tα1组,未接受Tα1治疗的患者;短期Tα1组,从治疗开始至CCRT结束每周接受一次Tα1(1.6 mg)治疗;长期Tα1组,从治疗开始至CCRT后12个月每周接受一次Tα1(1.6 mg)治疗。主要终点是无进展生存期(PFS)。次要终点包括总生存期(OS)、肺炎、循环淋巴细胞计数和白细胞介素-6(IL-6)水平。收集治疗前活检样本,以评估体细胞突变对治疗结果的潜在影响。
非Tα1组、短期Tα1组和长期Tα1组分别包括48例、101例和47例患者。CCRT后,各组分别有77.1%、75.2%和93.6%的患者符合巩固性纳武单抗治疗条件(P=0.03)。非Tα1组的中位PFS为14.6个月[95%置信区间(CI):11.9-17.3],短期Tα1组为16.0个月(95%CI:13.2-18.8),长期Tα1组未达到(P=0.03)。非Tα1组的中位OS为20.0个月(95%CI:16.1-23.9),短期Tα1组为27.6个月(95%CI:13.8-41.3),长期Tα1组未达到(P=0.01)。长期Tα1组≥2级肺炎的发生率显著较低(非Tα1组为35.4%,长期Tα1组为14.5%,P=0.02),CCRT后6个月淋巴细胞减少的发生率也较低(非Tα1组为55.8%,短期Tα1组为30.9%,长期Tα1组为22.5%,P=0.01)。CCRT后2个月,非Tα1组的中位IL-6水平(8.14 pg/mL)显著高于长期Tα1组(4.92 pg/mL,P=0.03)。
将Tα1纳入CCRT和巩固性免疫治疗对LA-NSCLC患者可能具有协同作用。这种联合治疗可能提高生存结局并降低治疗相关毒性。有必要进行进一步的随机试验以验证。