Martinez-Cajas Jorge L, Alvarado Beatriz, Jolly Ann, Gong Yanping, Stoner Bradley, Evans Gerald, Perez-Patrigeon Santiago, Guan T Hugh
Division of Infectious Diseases, Department of Medicine, Queen's University, Kingston, Ontario, Canada.
Department of Public Health Sciences. Queen's University, Kingston, Ontario, Canada.
PLoS One. 2025 Aug 13;20(8):e0303813. doi: 10.1371/journal.pone.0303813. eCollection 2025.
We established a longitudinal cohort of healthcare workers (HCWs) in an acute care hospital (ACH) and four long-term care homes (LTCHs) in Ontario, Canada, to follow the incidence of SARS-CoV-2 infection, humoral immune response to infection and/or vaccination, and determinants of infection risk. Here, we 1) describe the cohort regarding the distribution of main exposures, outcomes and serologic assays, 2) describe the unadjusted incidence of SARS-CoV-2 infection risk in the overall population, and 3) summarize the analysis and its pertinence.
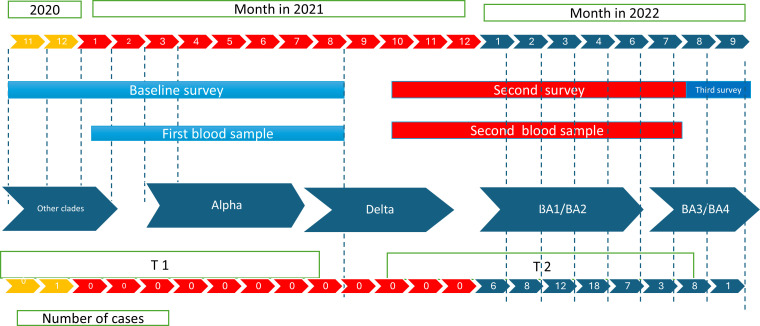
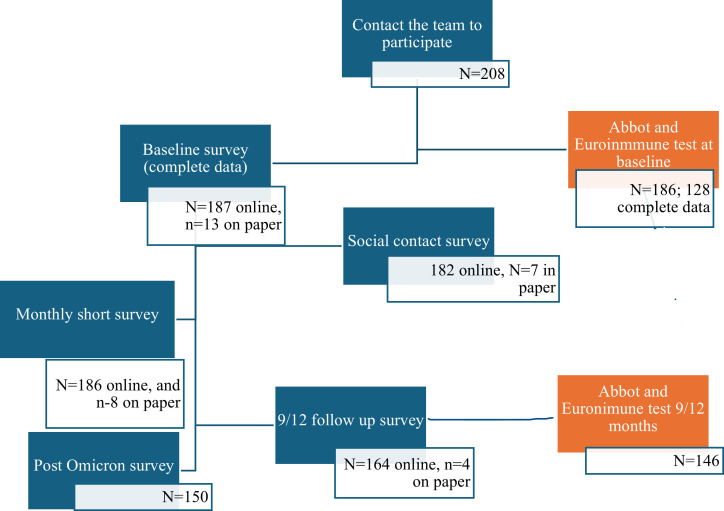
HCWs were recruited between November 24, 2020, and July 24, 2021. They completed a baseline survey, monthly surveillance for 9-12 months, a post-Omicron-wave survey, and provided blood samples for anti-SARS-CoV-2 antibody measurements. We collected data on host-related (humoral response to vaccines and SARS-CoV-2 infection) and environmental factors (social contact history and occupational, household and community conditions). Descriptive analysis by setting, comparison of distributions, and unadjusted survival analysis were performed.
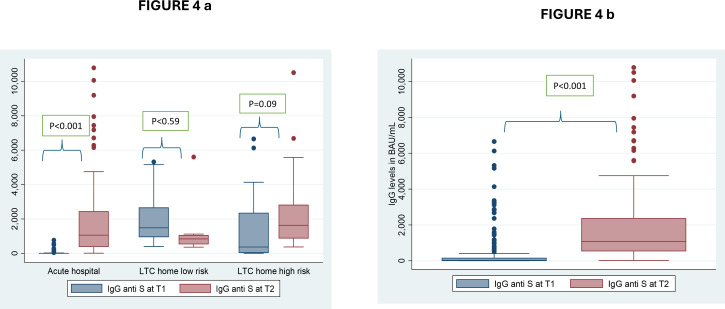
In total, 143 HCWs from the ACH and 57 from LTCHs had complete data, and 72% were followed until September 2022. Nearly 60% of the sample consisted of nurses, nurse assistants and personal support workers. Survival analysis showed that the risk of infection was bimodal, with low risk throughout the study period until the first Omicron wave. ACH HCWs had a higher risk of infection during the Omicron waves than during the preceding waves (Odds Ratio = 7.64; CI95%: 4.24-13.7), while LTCH HCWs at high-risk facilities experienced a similar risk of infection before and during the Omicron waves (OR = 1.76; CI95%: 0.63-4.9). During the Omicron waves, the use of protective equipment by HCWs working with institutional COVID-19 cases increased, but the use of community protective measures diminished. Household infections reported by participating HCWs also increased during the Omicron waves compared to previous waves. Immunoglobulin G (IgG) antibody levels increased over two time periods, (Pre vs Post- Omicron) likely due to the immune response to high levels of both vaccination and SARS-CoV-2 infections.
We observed a low incidence of COVID-19 until the onset of the Omicron waves, which highlights the drastic impact of this Variants of Concern (VOC) on transmission and the importance of infectious agent characteristics. Our analysis indicated a ninefold increased risk of infection compared to that in earlier pandemic periods. Further analysis will allow the estimation of 1) the risk factors for SARS-CoV-2 infection at the community, household and healthcare facility levels, 2) the relationship between humoral responses and SARS-CoV-2 infection/vaccination, and 3) the role of social contact in work, household and community settings in the risk of infection.
我们在加拿大安大略省的一家急症护理医院(ACH)和四家长期护理院(LTCH)中建立了一个医护人员纵向队列,以跟踪严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染的发生率、对感染和/或疫苗接种的体液免疫反应以及感染风险的决定因素。在此,我们1)描述该队列在主要暴露因素、结局和血清学检测方面的分布情况,2)描述总体人群中SARS-CoV-2感染风险的未调整发病率,3)总结分析及其相关性。
医护人员于2020年11月24日至2021年7月24日期间招募。他们完成了一项基线调查、为期9至12个月的月度监测、一次奥密克戎浪潮后调查,并提供血液样本用于检测抗SARS-CoV-2抗体。我们收集了与宿主相关的(对疫苗和SARS-CoV-2感染的体液反应)和环境因素(社交接触史以及职业、家庭和社区状况)的数据。进行了按机构设置的描述性分析、分布比较以及未调整的生存分析。
ACH的143名医护人员和LTCH的57名医护人员拥有完整数据,72%的人员随访至2022年9月。近60%的样本由护士、护士助理和个人支持工作者组成。生存分析表明,感染风险呈双峰模式,在整个研究期间直至首次奥密克戎浪潮期间风险较低。ACH的医护人员在奥密克戎浪潮期间的感染风险高于前几波(优势比=7.64;95%置信区间:4.24 - 13.7),而高危设施的LTCH医护人员在奥密克戎浪潮之前和期间经历的感染风险相似(优势比=1.76;95%置信区间:0.63 - 4.9)。在奥密克戎浪潮期间,与机构内新冠病例接触的医护人员使用防护设备的情况增加,但社区防护措施的使用减少。与前几波相比,参与研究的医护人员报告的家庭感染在奥密克戎浪潮期间也有所增加。免疫球蛋白G(IgG)抗体水平在两个时间段内升高(奥密克戎之前与之后),这可能是由于对高水平疫苗接种和SARS-CoV-2感染的免疫反应。
在奥密克戎浪潮开始之前,我们观察到新冠病毒病(COVID-19)的发病率较低,这凸显了这种关注变异株(VOC)对传播的巨大影响以及传染源特征的重要性。我们的分析表明,与早期大流行时期相比,感染风险增加了九倍。进一步的分析将有助于估计1)社区、家庭和医疗机构层面SARS-CoV-2感染的风险因素,2)体液反应与SARS-CoV-2感染/疫苗接种之间的关系,以及3)工作、家庭和社区环境中的社交接触在感染风险中的作用。