Halman Joanna, Elshof Jan-Willem, Bieniaszewski Ksawery, Bieniaszewski Leszek, Zielińska Natalia, Wójcikiewicz Adam, Dźwil Mateusz, Znaniecki Łukasz, Targoński Radosław
Department of Vascular Surgery, University Clinical Center and Faculty of Medicine, Medical University of Gdańsk, 80-214 Gdańsk, Poland.
Department of Vascular Surgery, VieCuri Medisch Centrum, 5912 BL Venlo, The Netherlands.
J Clin Med. 2025 Jul 28;14(15):5333. doi: 10.3390/jcm14155333.
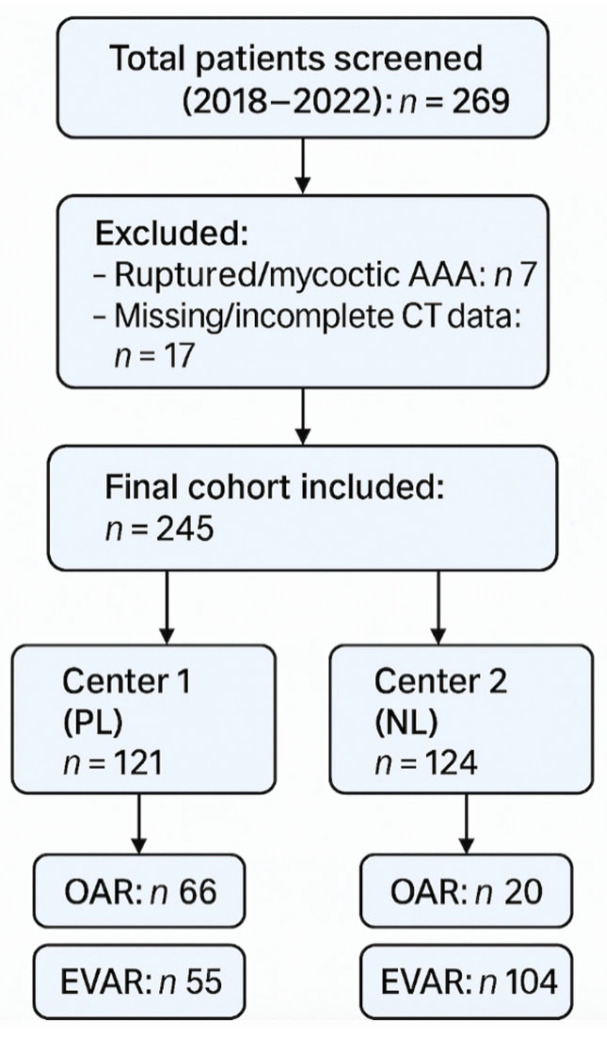
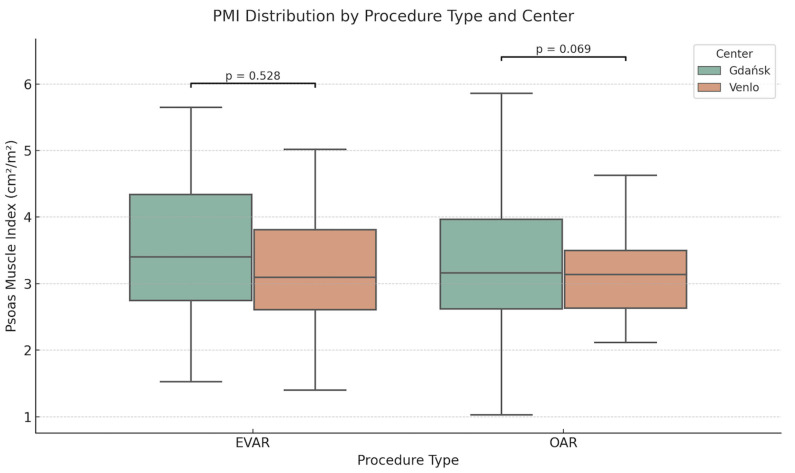
Sarcopenia is a predictor of poor surgical outcomes in older adults. The Psoas Muscle Index (PMI), calculated from routine preoperative CT scans, has been proposed as an imaging-based marker of physiological reserve, but its diagnostic utility in vascular surgery remains unclear. We aimed to assess the predictive value of PMI for early complications following elective abdominal aortic aneurysm (AAA) repair in two European centers. We retrospectively analyzed 245 patients who underwent open or endovascular AAA repair between 2018 and 2022 in Poland and The Netherlands. PMI was measured at the level of third lumbar vertebrae (L3) level, normalized to height, and stratified into center-specific tertiles. Early complications were compared across tertiles, procedures, and centers. Multivariate logistic regression was used to adjust for age, comorbidities, and procedure type. Low PMI was significantly associated with early complications in EVAR patients at the Polish center ( = 0.004). No associations were found in open repair or at the Dutch center. Mean PMI values did not differ significantly between centers. PMI may serve as a context-dependent imaging biomarker for early risk stratification following AAA repair, particularly in endovascular cases. Its predictive value is influenced by institutional and procedural factors, highlighting the need for prospective validation and standardization before clinical adoption.
肌肉减少症是老年人手术预后不良的一个预测指标。根据术前常规CT扫描计算得出的腰大肌指数(PMI),已被提议作为基于影像学的生理储备指标,但其在血管外科手术中的诊断效用仍不明确。我们旨在评估在两个欧洲中心,PMI对择期腹主动脉瘤(AAA)修复术后早期并发症的预测价值。我们回顾性分析了2018年至2022年期间在波兰和荷兰接受开放或血管腔内AAA修复术的245例患者。在第三腰椎(L3)水平测量PMI,并根据身高进行标准化,然后按中心特异性三分位数进行分层。比较了三分位数、手术方式和中心之间的早期并发症情况。采用多因素逻辑回归分析对年龄、合并症和手术类型进行校正。在波兰中心,低PMI与血管腔内修复术(EVAR)患者的早期并发症显著相关(P = 0.004)。在开放修复组或荷兰中心未发现相关性。各中心之间的平均PMI值无显著差异。PMI可作为AAA修复术后早期风险分层的一种依赖于具体情况的影像学生物标志物,尤其是在血管腔内修复病例中。其预测价值受机构和手术因素的影响,这突出表明在临床应用前需要进行前瞻性验证和标准化。