Suartz Caio Vinicius, de Lima Richard Dobrucki, de Almeida Lucas Schenk, Liebl Bruno, Lopes Roberto Iglesias, Branquinho Reis Gabriel Baêta, Henry Sant'Anna Pedro Vasconcelos, Faris de Campos Vinícius Daniel, Mota José Mauricio, Lima Aguiar Melão Bárbara Vieira, Nahas William Carlos, Shahrour Walid, Shabana Walid, Ribeiro-Filho Leopoldo Alves, Toren Paul, Fradet Vicent
Department of Urology, Thunder Bay Regional Health Sciences Centre and Northern Ontario School of Medicine University, Thunder Bay, ON, Canada.
Urology Department, CHU de Québec-Université Laval, Quebec City, QC, Canada.
Eur Urol Open Sci. 2025 Aug 6;79:45-59. doi: 10.1016/j.euros.2025.07.010. eCollection 2025 Sep.
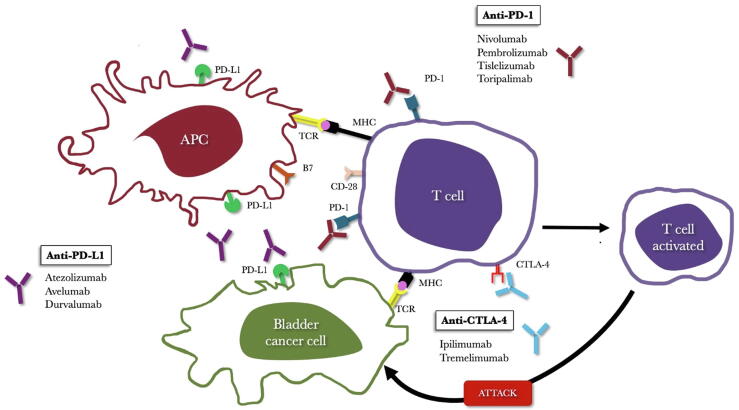
Immune checkpoint inhibitors (ICIs), alone or with platinum-based chemotherapy, have increasingly been studied as neoadjuvant therapy for muscle-invasive bladder cancer (BC). We sought to evaluate the current evidence about neoadjuvant immunotherapy for BC.
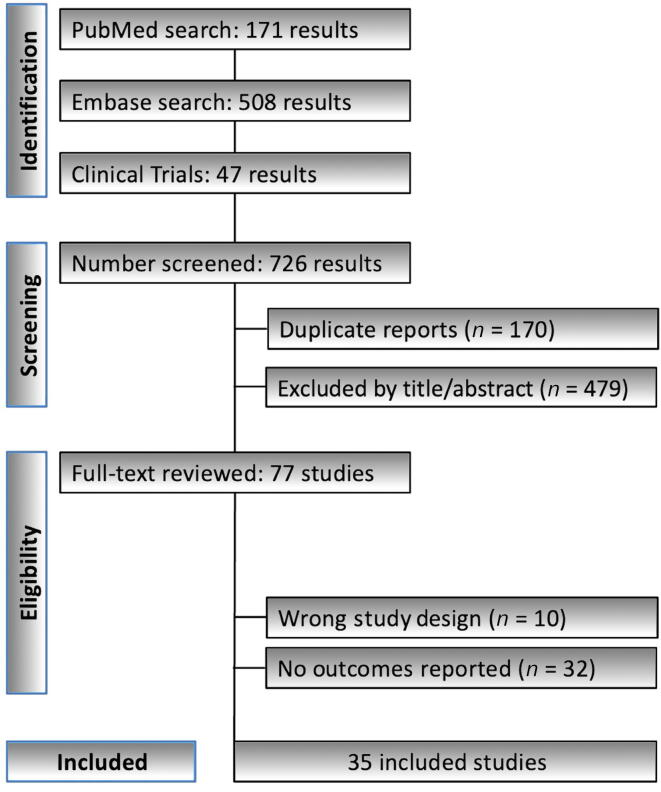
In this systematic review, conducted in October 2024, only prospective studies on neoadjuvant immunotherapy for BC were included. Extracted variables encompassed study design, clinical-pathological characteristics, perioperative outcomes, pathological complete response (pCR) rates, overall survival (OS), event-free survival, and immune-related (irAEs) and treatment-related (TRAEs) adverse events.
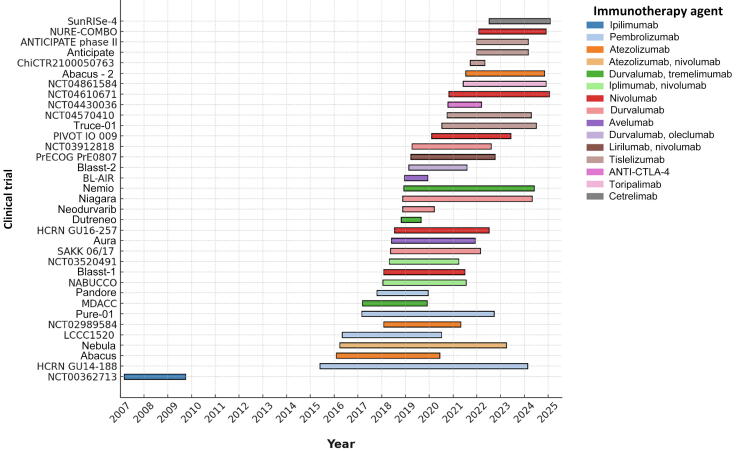
From 726 records, 35 studies met the inclusion criteria. The highest pCR rate observed was 54%, utilizing durvalumab. Perioperative chemoimmunotherapy with durvalumab plus cisplatin/gemcitabine showed greater OS than chemotherapy alone in the NIAGARA trial. The NEMIO trial achieved the highest 12-mo OS rate of 97%, using durvalumab in combination with tremelimumab and dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin, followed by the AURA trial (95%) and the LCCC1520 trial (91%). At 24 mo, the NEBULA trial reported a 100% OS rate with three doses of atezolizumab, while PrECOG PrE0807 reached and OS rate of 89% with nivolumab and lirilumab. The highest rates of grade 3 and 4 irAEs were reported for nivolumab combined with ipilimumab (54%) and for durvalumab combined with tremelimumab (64%). The most common grade 3/4 irAEs were hepatitis (2-27%), kidney injury (2-100%), and skin rash (1.1-41%). Grade 3/4 TRAEs were comparable between the ICI and chemotherapy groups.
Neoadjuvant immunotherapy for BC has shown promising efficacy and a manageable adverse event profile. However, financial toxicity, the absence of predictive biomarkers, and the risk of significant irAEs remain challenges.
This study reviewed recent clinical trials that tested immunotherapy before surgery in patients with bladder cancer. The results suggest that a combination of immunotherapy and chemotherapy may improve outcomes and reduce the risk of cancer returning. These findings could help shape future treatment options for patients with muscle-invasive bladder cancer.
免疫检查点抑制剂(ICI)单独或与铂类化疗联合,越来越多地被作为肌肉浸润性膀胱癌(BC)的新辅助治疗进行研究。我们旨在评估目前关于BC新辅助免疫治疗的证据。
在2024年10月进行的这项系统评价中,仅纳入了关于BC新辅助免疫治疗的前瞻性研究。提取的变量包括研究设计、临床病理特征、围手术期结果、病理完全缓解(pCR)率、总生存期(OS)、无事件生存期、免疫相关(irAE)和治疗相关(TRAE)不良事件。
从726条记录中,35项研究符合纳入标准。观察到的最高pCR率为54%,使用的是度伐利尤单抗。在NIAGARA试验中,度伐利尤单抗联合顺铂/吉西他滨的围手术期化疗免疫疗法显示出比单纯化疗更长的OS。NEMIO试验使用度伐利尤单抗联合曲美木单抗和剂量密集的甲氨蝶呤、长春碱、多柔比星和顺铂,达到了最高的12个月OS率97%,其次是AURA试验(95%)和LCCC1520试验(91%)。在24个月时,NEBULA试验报告三剂阿替利珠单抗的OS率为100%,而PrECOG PrE0807试验使用纳武利尤单抗和利鲁单抗达到了89%的OS率。纳武利尤单抗联合伊匹木单抗(54%)和度伐利尤单抗联合曲美木单抗(64%)报告的3/4级irAE发生率最高。最常见的3/4级irAE是肝炎(2%-27%)、肾损伤(2%-100%)和皮疹(1.1%-41%)。ICI组和化疗组之间3/4级TRAE相当。
BC新辅助免疫治疗已显示出有前景的疗效和可管理的不良事件特征。然而,经济毒性、缺乏预测生物标志物以及严重irAE的风险仍然是挑战。
本研究回顾了近期在膀胱癌患者手术前测试免疫疗法的临床试验。结果表明,免疫疗法和化疗联合可能改善预后并降低癌症复发风险。这些发现可能有助于为肌肉浸润性膀胱癌患者制定未来的治疗方案。