Cangiano Lorenzo, Bonomi Alice, Cosentino Nicola, Leoni Olivia, Trombara Filippo, Myasoedova Veronika A, Poggio Paolo, Trabattoni Daniela, Agostoni Piergiuseppe, Marenzi Giancarlo
Centro Cardiologico Monzino Istituto di Ricovero e Cura a Carattere Scientifico, Milan, Italy.
Regione Lombardia, Milan, Italy.
Open Heart. 2025 Aug 18;12(2):e003517. doi: 10.1136/openhrt-2025-003517.
Women with acute myocardial infarction (AMI) experience higher mortality rates than men. This disparity is influenced by factors such as older age, greater comorbidity burden, atypical symptom presentation and delays in treatment. This study analysed patients with AMI (2003-2018) from the Lombardy Health Database (Italy) to examine sex differences in in-hospital and 1-year mortality and the role of age, percutaneous coronary intervention (PCI) and postdischarge therapy.
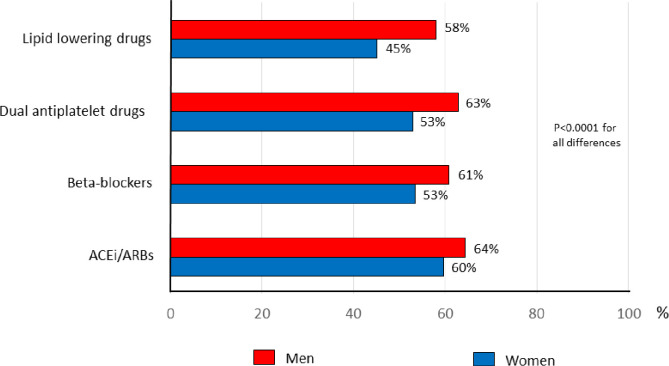
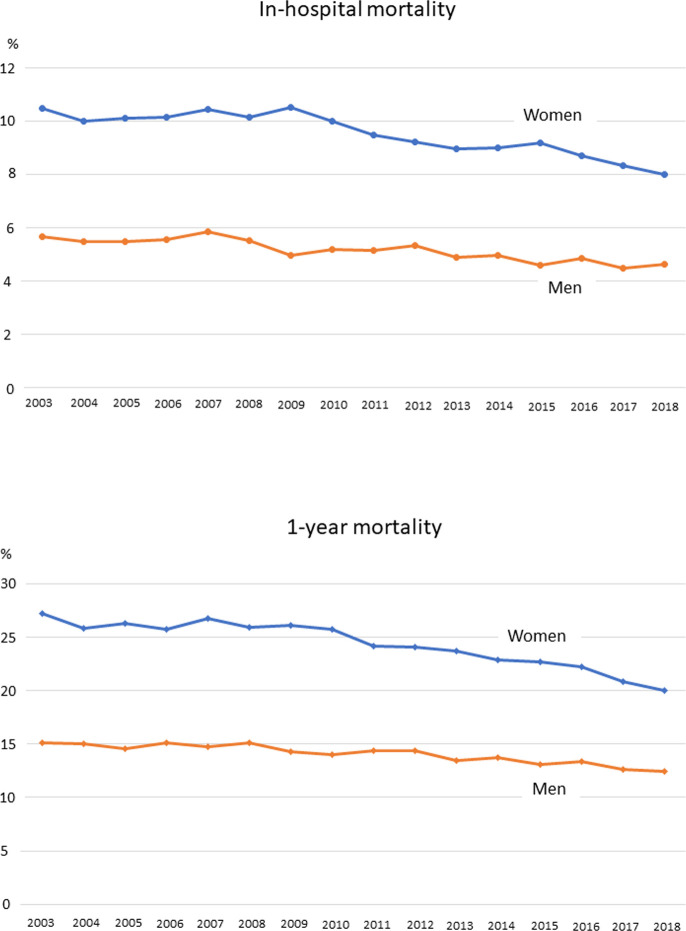
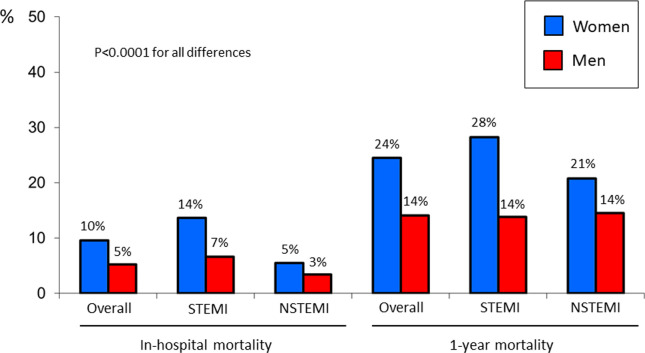
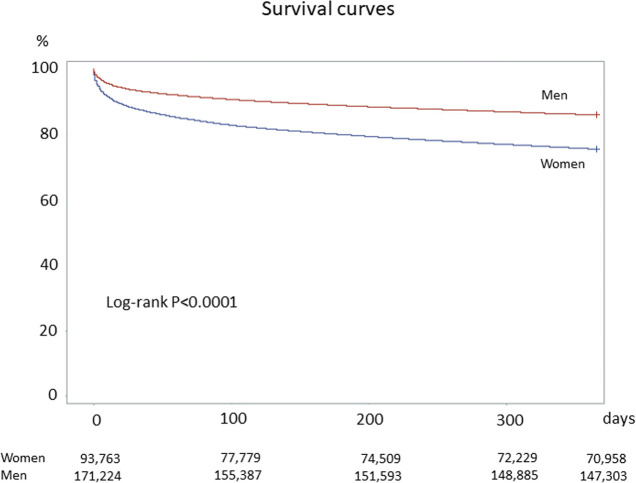
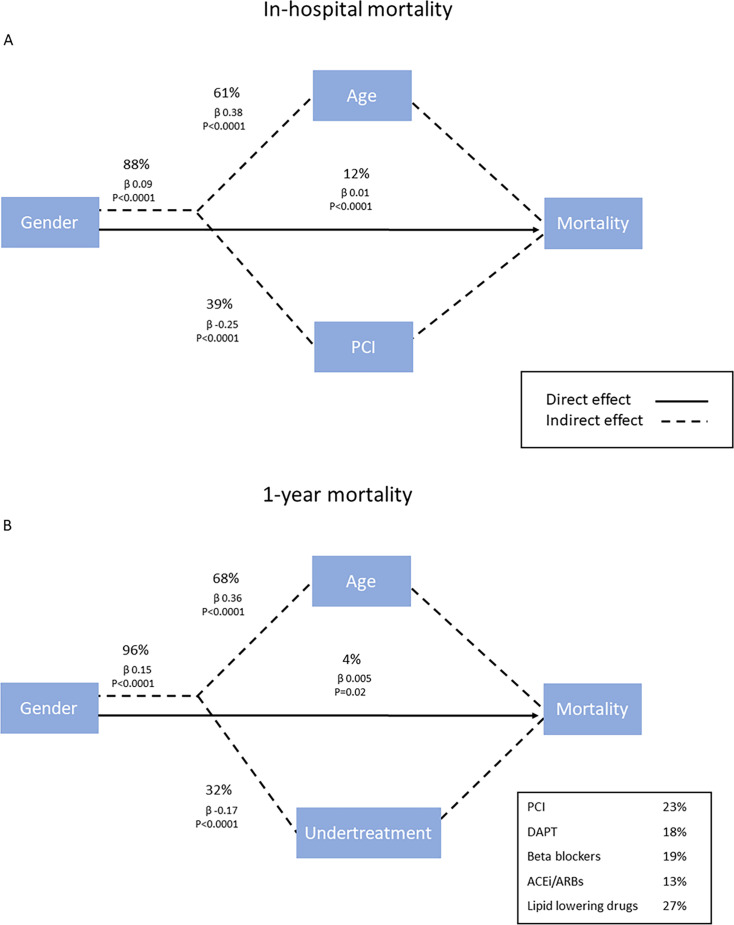
Among 263 564 patients with AMI (93 363 women, 170 201 men), primary and secondary endpoints were in-hospital and 1-year mortality, respectively. Path analysis evaluated the direct and indirect effects of sex on outcomes, incorporating age, PCI and postdischarge therapy as mediators. Women had higher in-hospital (10% vs 5%; p<0.0001) and 1-year mortality (24% vs 14%; p<0.0001) but were less likely to receive PCI (40% vs 61%; p<0.0001) and postdischarge therapy (dual antiplatelet therapy 53% vs 63%; ACE inhibitors/angiotensin receptor blockers 60% vs 64%; beta blockers 53% vs 61%; lipid-lowering drugs 45% vs 58%; p<0.0001 for all differences). After adjusting for age, major comorbidities, PCI and postdischarge treatment, mortality differences were no longer significant (adjusted OR 1.04; 95% CI 0.99 to 1.07 for in-hospital mortality) or even reversed (adjusted HR 0.94; 95% CI 0.92 to 0.96 for 1-year mortality). Path analysis showed that female sex directly contributed 12% to in-hospital mortality and 4% to 1-year mortality, while age and undertreatment accounted for most of the disparity (88% and 96%, respectively).
Women with AMI face higher mortality largely due to older age and undertreatment during hospitalisation and after discharge. Addressing these gaps could improve outcomes.
急性心肌梗死(AMI)女性患者的死亡率高于男性。这种差异受多种因素影响,如年龄较大、合并症负担较重、症状不典型以及治疗延迟。本研究分析了伦巴第健康数据库(意大利)中2003年至2018年的AMI患者,以研究住院期间及1年死亡率的性别差异,以及年龄、经皮冠状动脉介入治疗(PCI)和出院后治疗的作用。
在263564例AMI患者(93363例女性,170201例男性)中,主要终点和次要终点分别为住院期间死亡率和1年死亡率。路径分析评估了性别对结局的直接和间接影响,将年龄、PCI和出院后治疗作为中介因素。女性的住院死亡率(10%对5%;p<0.0001)和1年死亡率(24%对14%;p<0.0001)较高,但接受PCI治疗的可能性较小(40%对61%;p<0.0001),出院后治疗的情况也是如此(双联抗血小板治疗53%对63%;血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂60%对64%;β受体阻滞剂53%对61%;降脂药物45%对58%;所有差异p<0.0001)。在调整年龄、主要合并症、PCI和出院后治疗因素后,死亡率差异不再显著(住院死亡率调整后的比值比为1.04;95%置信区间为0.99至1.07),甚至出现逆转(1年死亡率调整后的风险比为0.94;95%置信区间为0.92至0.96)。路径分析表明,女性性别对住院死亡率的直接贡献率为12%,对1年死亡率的直接贡献率为4%,而年龄和治疗不足占差异的大部分(分别为88%和96%)。
AMI女性患者死亡率较高,主要是由于年龄较大以及住院期间和出院后治疗不足。解决这些差距可能会改善预后。