Wu Yeshun, Tu Xiaoming, Jin Qizhi, Zheng Jiasheng, Gao Zhenyan
Department of Cardiology, Quzhou Affiliated Hospital of Wenzhou Medical University Quzhou People's Hospital, Quzhou, China.
Ann Med Surg (Lond). 2025 May 26;87(7):4096-4104. doi: 10.1097/MS9.0000000000003362. eCollection 2025 Jul.
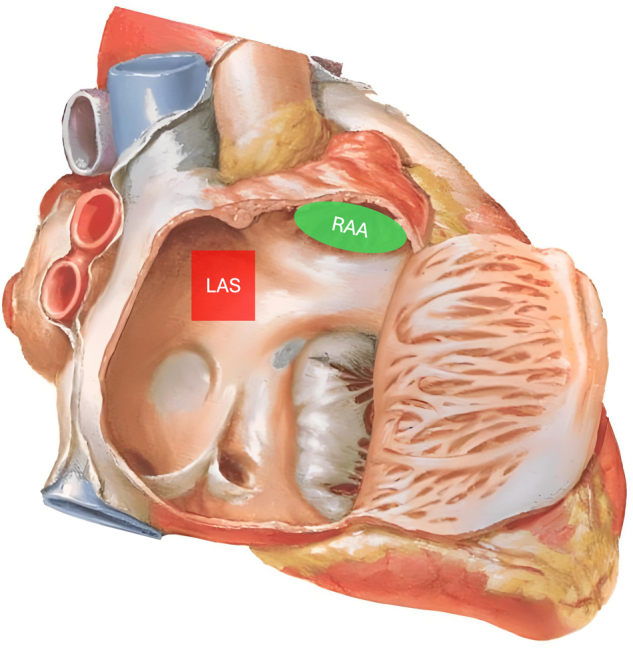
Patients with sinus node dysfunction (SND) are at risk of atrial fibrillation (AF) after dual-chamber pacemaker implantation. AF is a risk factor for cardiovascular and cerebrovascular events. The location of atrial electrodes can influence AF occurrence. This study aimed to investigate the differences in the incidence of new-onset AF between low atrial septal (LAS) and right atrial appendage (RAA) pacing in patients with SND and explore the possible underlying mechanisms.
We included 155 patients with SND, including 83 and 72 who received LAS and RAA pacing, respectively. We collected baseline data, electrocardiogram indexes, and ultrasound cardiogram indexes, as well as postoperative complications, program testing data of the pacemaker, electrocardiogram indexes, and AF occurrence during 1-year follow-up.
The operative duration was significantly longer in the LAS group than in the RAA group ( 0.001). The intraoperative P-wave amplitude was significantly smaller in the LAS group than in the RAA group (0.001). The P-wave duration and cumulative percentages of ventricular pacing (Cum % VP) in the LAS group were significantly lower than those in the RAA group ( 0.001 and 0.039, respectively). At 1-year follow-up, the incidence of new-onset AF was significantly lower in the LAS group than in the RAA group (16.9% vs. 36.1%, hazard ratio [HR]: 0.363, 95% confidence interval [CI]: 0.156-0.846, = 0.019). The independent risk factors for new-onset AF at 1-year follow-up were combined bundle branch block (odds ratio [OR] 8.015, 95% CI 1.232-52.132, = 0.029), large left atrium (OR 5.812, 95% CI 1.202-28.088, = 0.029), and prolonged postoperative P-wave duration (OR 1.027, 95% CI 1.009-1.045, = 0.018). LAS pacing was associated with a reduced risk of postoperative AF occurrence (OR 0.072, 95% CI 0.010-0.542, = 0.011).
For patients with SND after dual-chamber pacemaker implantation, AF incidence within 1 year after LAS pacing was significantly lower than that after RAA pacing. LAS pacing could shorten the postoperative P-wave duration, an independent risk factor for new-onset AF, and LAS pacing effectively reduced the Cum % VP, which may be the underlying mechanism by which LAS pacing prevents postoperative AF occurrence.
窦房结功能障碍(SND)患者在植入双腔起搏器后有发生心房颤动(AF)的风险。AF是心血管和脑血管事件的危险因素。心房电极的位置会影响AF的发生。本研究旨在调查SND患者低位房间隔(LAS)起搏与右心耳(RAA)起搏新发AF发生率的差异,并探讨可能的潜在机制。
我们纳入了155例SND患者,其中分别有83例和72例接受了LAS起搏和RAA起搏。我们收集了基线数据、心电图指标、超声心动图指标,以及术后并发症、起搏器程控测试数据、心电图指标和1年随访期间的AF发生情况。
LAS组的手术时间显著长于RAA组(P<0.001)。LAS组术中P波振幅显著小于RAA组(P<0.001)。LAS组的P波时限和心室起搏累积百分比(Cum % VP)显著低于RAA组(分别为P<0.001和P = 0.039)。在1年随访时,LAS组新发AF的发生率显著低于RAA组(16.9% 对36.1%,风险比[HR]:0.363,95%置信区间[CI]:0.156 - 0.846,P = 0.019)。1年随访时新发AF的独立危险因素为合并束支传导阻滞(比值比[OR] 8.015,95% CI 1.232 - 52.132,P = 0.029)、左心房增大(OR 5.812,95% CI 1.202 - 28.088,P = 0.029)和术后P波时限延长(OR 1.027,95% CI 1.009 - 1.045,P = 0.018)。LAS起搏与术后AF发生风险降低相关(OR 0.072,95% CI 0.010 - 0.542,P = 0.011)。
对于双腔起搏器植入术后的SND患者,LAS起搏后1年内AF发生率显著低于RAA起搏后。LAS起搏可缩短术后P波时限,这是新发AF的独立危险因素,且LAS起搏有效降低了Cum % VP,这可能是LAS起搏预防术后AF发生的潜在机制。