Zhang Mengmeng, Xu Rui, Wang Juan, Wu Chunyan, Ren Huicong, Zhang Zhaohui, Li Juan
Psychiatry Department, The Second Affiliated Hospital of Xinxiang Medical University, Xinxiang, China.
Henan Collaborative Innovation Center of Prevention and Treatment of Mental Disorder, Xinxiang Medical University, Xinxiang, China.
Front Psychiatry. 2025 Aug 12;16:1587179. doi: 10.3389/fpsyt.2025.1587179. eCollection 2025.
Although well-established as a first-line treatment for psychiatric disorders, electroconvulsive therapy (ECT) carries risks of adverse effects, including fever. The purpose of this study was to elucidate the incidence, clinical characteristics, and risk factors related to fever after ECT.
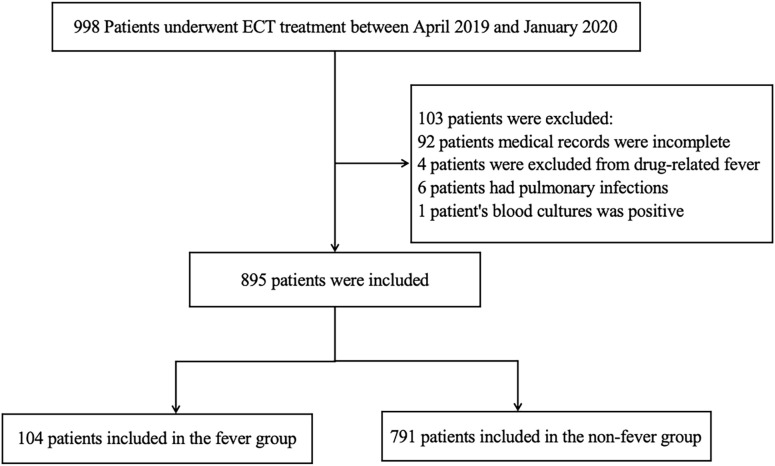
We retrospectively analyzed medical records of patients receiving ECT at the Second Affiliated Hospital of Xinxiang Medical University (April 2019-January 2020). Patients were subsequently divided into two groups: a fever group, in which the body temperature was ≥ 38°C; and a non-fever group, in which the body temperature was <38°C.
A total of 895 patients underwent 7801 units of ECT treatment. Fever was analyzed at the patient and treatment unit level. At the patient level, 104 out of 895 patients (11.6%) experienced at least one fever within 24 hours after ECT, Compared with the non-fever group, the fever group showed statistically significant differences in age, gender, types of psychiatric ward (closed or open), and anesthetic type (all < 0.05) but not in the total number of ECT units or diagnoses, Logistic regression analysis identified the risk variables for fever as younger age (≤ 29), closed psychiatric ward, etomidate administration, and being male; and at the treatment units level, among the 7,801 ECT units, fever occurred in 129 units (1.7%), with a median maximum temperature of 38.5 (38.0-40.3)°C. Following ECT, 55.8% (72/129) of the fever unit temperatures returned to normal body temperature as assessed by clinical observation or cooling measures, whereas 44.2% (57/129) required cooling combined with antibiotics. Compared to baseline, the fever units had higher white blood cell and neutrophil counts ( < 0.001) but lower lymphocyte counts ( < 0.001). In 79.8% (103/129) of the units, the fever was observed during the first 5-8 hours after the ECT treatment was completed, with 94.6% (122/129) of the units returning to normal body temperature within 24 hours of treatment. Only 5.4% (7/129) of the units opted to discontinue ECT treatment due to fever.
We found that fever after ECT requires attention in clinical practice. Although the direct impact of fever after ECT treatment is limited, given its potential risks, it is advised to focus on strengthening the temperature monitoring of high-risk groups.
尽管电休克疗法(ECT)作为精神疾病的一线治疗方法已被广泛认可,但它存在包括发热在内的不良反应风险。本研究的目的是阐明ECT后发热的发生率、临床特征及相关危险因素。
我们回顾性分析了新乡医学院第二附属医院2019年4月至2020年1月接受ECT治疗的患者的病历。随后将患者分为两组:发热组,体温≥38°C;非发热组,体温<38°C。
共有895例患者接受了7801次ECT治疗。在患者和治疗单元层面分析发热情况。在患者层面,895例患者中有104例(11.6%)在ECT后24小时内至少经历一次发热。与非发热组相比,发热组在年龄、性别、精神科病房类型(封闭式或开放式)和麻醉类型方面均有统计学显著差异(均<0.05),但在ECT治疗次数或诊断方面无差异。逻辑回归分析确定发热的风险变量为年龄较小(≤29岁)、封闭式精神科病房、使用依托咪酯和男性;在治疗单元层面,在7801次ECT治疗中,129次(1.7%)出现发热,最高体温中位数为38.5(38.0 - 40.3)°C。ECT后,通过临床观察或降温措施评估,72次(55.8%)发热治疗单元的体温恢复正常,而57次(44.2%)需要联合使用抗生素降温。与基线相比,发热治疗单元的白细胞和中性粒细胞计数较高(<0.001),但淋巴细胞计数较低(<0.001)。在79.8%(103/129)的治疗单元中,发热出现在ECT治疗完成后的前5 - 8小时,94.6%(122/129)的治疗单元在治疗后24小时内体温恢复正常。仅5.4%(7/129)的治疗单元因发热而停止ECT治疗。
我们发现ECT后发热在临床实践中需要引起关注。尽管ECT治疗后发热的直接影响有限,但鉴于其潜在风险,建议重点加强对高危人群的体温监测。