Aoki Kazuyasu, Mayahara Taku, Katayama Tomohiro, Hirai Yuya, Uchihashi Masao, Fukuoka Ryosuke
Department of Emergency and General Medicine, Kobe Ekisaikai Hospital, 1-21-1 Manabigaoka, Kobe, Tarumi-ku, Hyogo, 655-0004, Japan.
Department of Anesthesiology, Kobe Ekisaikai Hospital, Kobe, Japan.
JA Clin Rep. 2025 Aug 29;11(1):47. doi: 10.1186/s40981-025-00812-w.
Guidelines recommend prophylactic chest tube placement in patients with traumatic pneumothorax who require positive pressure ventilation to prevent tension pneumothorax. However, chest tube insertion is not without complications, and avoiding it when safely possible is desirable.
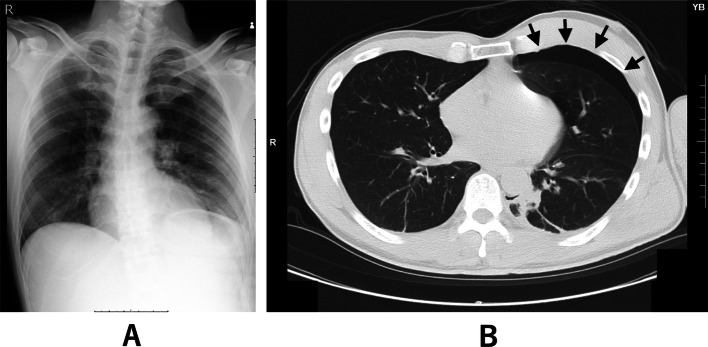
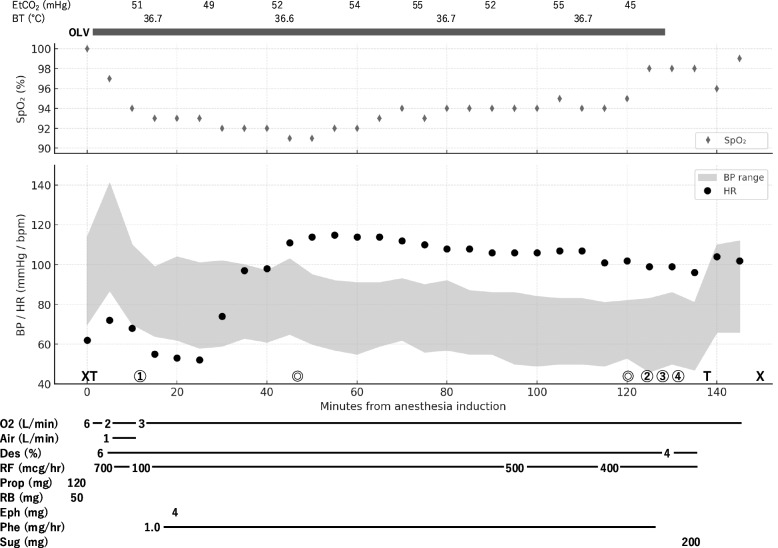
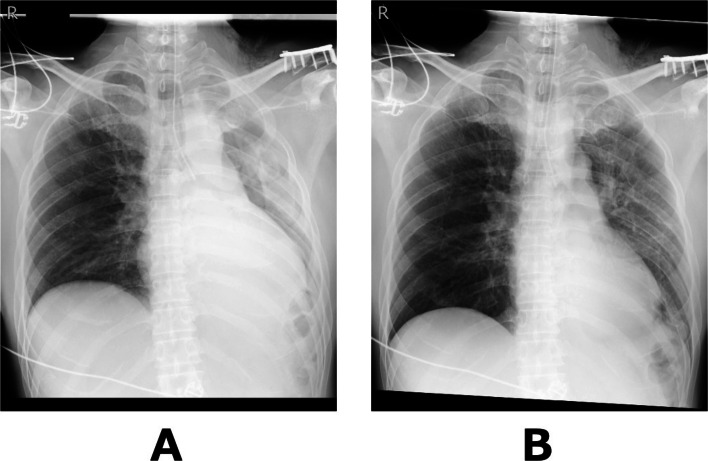
A man in his 50 s with a left clavicle fracture and mild left-sided occult pneumothorax on computed tomography was scheduled for surgery under general anesthesia. Conservative management was chosen given the absence of respiratory symptoms and stable imaging. To minimize the risk of pneumothorax progression during positive pressure ventilation, one-lung ventilation was employed to avoid ventilating the affected lung. Surgery proceeded uneventfully, with transient hypoxemia that was managed by increasing FiO to 100%. Postoperative imaging confirmed re-expansion of the left lung and no pneumothorax progression. The patient was discharged in good condition.
General anesthesia was safely managed without prophylactic chest tube placement by employing one-lung ventilation in a patient with occult traumatic pneumothorax.
指南建议,对于需要进行正压通气的创伤性气胸患者,应预防性放置胸管以预防张力性气胸。然而,胸管插入并非没有并发症,在安全可行的情况下避免插入胸管是可取的。
一名50多岁男性,因左锁骨骨折,计算机断层扫描显示左侧轻度隐匿性气胸,计划在全身麻醉下进行手术。鉴于无呼吸道症状且影像学表现稳定,选择了保守治疗。为尽量降低正压通气期间气胸进展的风险,采用单肺通气以避免对患侧肺进行通气。手术顺利进行,出现短暂低氧血症,通过将吸入氧浓度提高到100%进行处理。术后影像学检查证实左肺复张且气胸无进展。患者康复出院。
对于隐匿性创伤性气胸患者,通过采用单肺通气,在未预防性放置胸管的情况下安全实施了全身麻醉。