Woods Kate, Beidas Mustafa, Murugan Vikram, Billion Taylor, Tauseef Abubakar, Mirza Mohsin
Creighton University School of Medicine, Omaha, NE, USA.
Department of Internal Medicine, Creighton University, Omaha, NE, USA.
Respir Res. 2025 Sep 1;26(1):267. doi: 10.1186/s12931-025-03336-0.
Lung cancer is the most frequent cause of cancer-related deaths in the United States and worldwide. Infectious diseases such as pneumonia and influenza are major risk factors for morbidity and mortality in patients diagnosed with lung cancer. Our study expands upon existing literature investigating epidemiological differences in lung cancer mortality, using the Centers for Disease Control and Prevention (CDC) Wide-ranging Online Data for Epidemiology Research (WONDER) database to report on influenza- and pneumonia-related mortality rates in lung cancer patients through multiple decades.
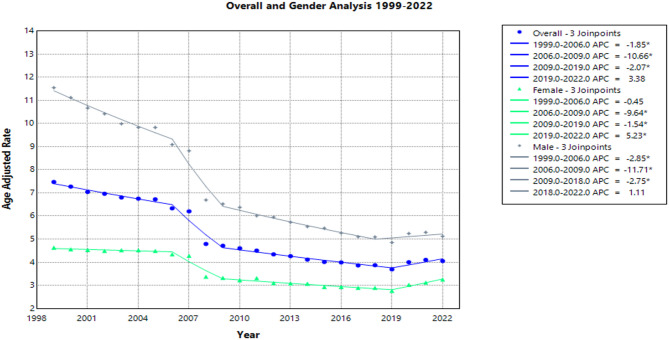
CDC WONDER was used to identify influenza- and pneumonia-related deaths in lung cancer patients that occurred within the United States from 1999 to 2022. Crude and age-adjusted mortality rates (AAMR) were calculated, as well as annual percent change and weighted average annual percent change with 95% confidence intervals for the AAMRs. The Joinpoint Regression Program was used to determine trends in mortality within the study period.
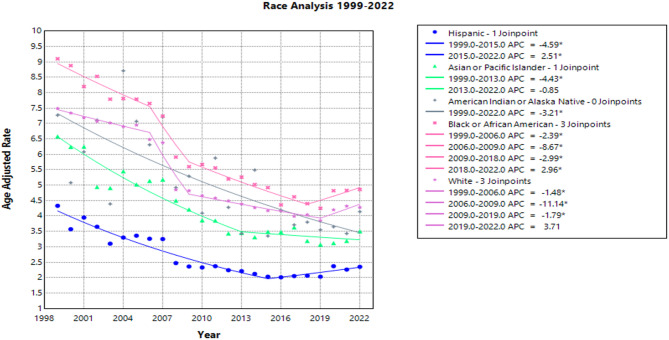
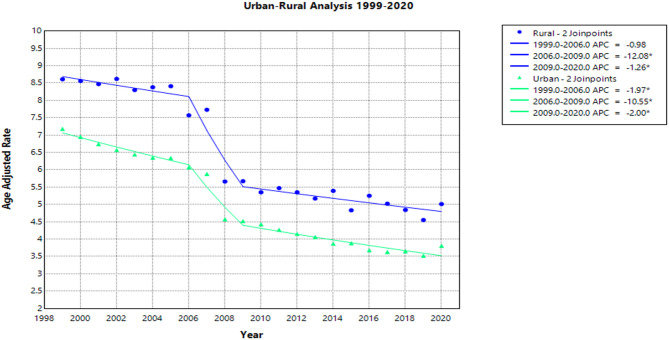
From 1999 to 2022, male lung cancer patients demonstrated greater mortality rates from pneumonia and influenza compared to females (60.6% vs. 39.4%). When stratified by race and ethnicity, Black patients had the highest AAMR over the study period at 9.1 per 100,000 people in 1999, as well as the most significant reduction in AAMR to 4.9 per 100,000 people in 2022. Additionally, AAMRs were consistently higher in rural areas compared to urban locations. By age group, patients aged 75–84 had the highest overall crude mortality rate at 28.3 per 100,000 people in 1999, with the lowest rate in ages 35–44 at 0.2 per 100,000 people in 2022.
This study expands upon previously reported trends in lung cancer mortality, highlighting epidemiological differences in influenza- and pneumonia-related death. Significant disparities in mortality rates were noted in older-aged, male, Black, and rural lung cancer patients. Targeted public health strategies concerning the unique needs of these diverse populations will be essential in improving mortality rates. Future research should also investigate the underlying causes of these disparities, and examine how certain community-based initiatives, such as campaigns for tobacco cessation, vaccination, and lung cancer screening, can inform guidelines and reduce preventable mortality in high-risk groups.
The online version contains supplementary material available at 10.1186/s12931-025-03336-0.
肺癌是美国和全球癌症相关死亡的最常见原因。肺炎和流感等传染病是肺癌患者发病和死亡的主要危险因素。我们的研究扩展了现有文献,通过使用疾病控制与预防中心(CDC)的广泛在线流行病学研究数据(WONDER)数据库,调查肺癌死亡率的流行病学差异,以报告数十年来肺癌患者中与流感和肺炎相关的死亡率。
使用CDC WONDER来确定1999年至2022年在美国发生的肺癌患者中与流感和肺炎相关的死亡。计算了粗死亡率和年龄调整死亡率(AAMR),以及年度百分比变化和AAMR的加权平均年度百分比变化及其95%置信区间。使用Joinpoint回归程序来确定研究期间的死亡率趋势。
1999年至2022年,男性肺癌患者的肺炎和流感死亡率高于女性(60.6%对39.4%)。按种族和族裔分层时,黑人患者在研究期间的AAMR最高,1999年为每10万人9.1例,到2022年AAMR下降幅度最大,降至每10万人4.9例。此外,农村地区的AAMR始终高于城市地区。按年龄组划分,75 - 84岁患者的总体粗死亡率最高,1999年为每10万人28.3例,35 - 44岁年龄组的死亡率最低,2022年为每10万人0.2例。
本研究扩展了先前报道的肺癌死亡率趋势,突出了与流感和肺炎相关死亡的流行病学差异。在老年、男性、黑人及农村肺癌患者中注意到死亡率存在显著差异。针对这些不同人群的独特需求制定有针对性的公共卫生策略对于提高死亡率至关重要。未来的研究还应调查这些差异的根本原因,并研究某些基于社区的举措,如戒烟运动、疫苗接种和肺癌筛查,如何为指南提供信息并降低高危人群中可预防的死亡率。
在线版本包含可在10.1186/s12931-025-03336-0获取的补充材料。