Herrera Nathaniel T, Ni Haibo, Smith Charlotte E R, Wu Yixuan, Dobrev Dobromir, Morotti Stefano, Grandi Eleonora
Department of Pharmacology, University of California Davis, Davis, California, United States.
Institute of Pharmacology, West German Heart and Vascular Center, University Duisburg-Essen, Essen, Germany.
bioRxiv. 2025 Aug 22:2025.08.18.670886. doi: 10.1101/2025.08.18.670886.
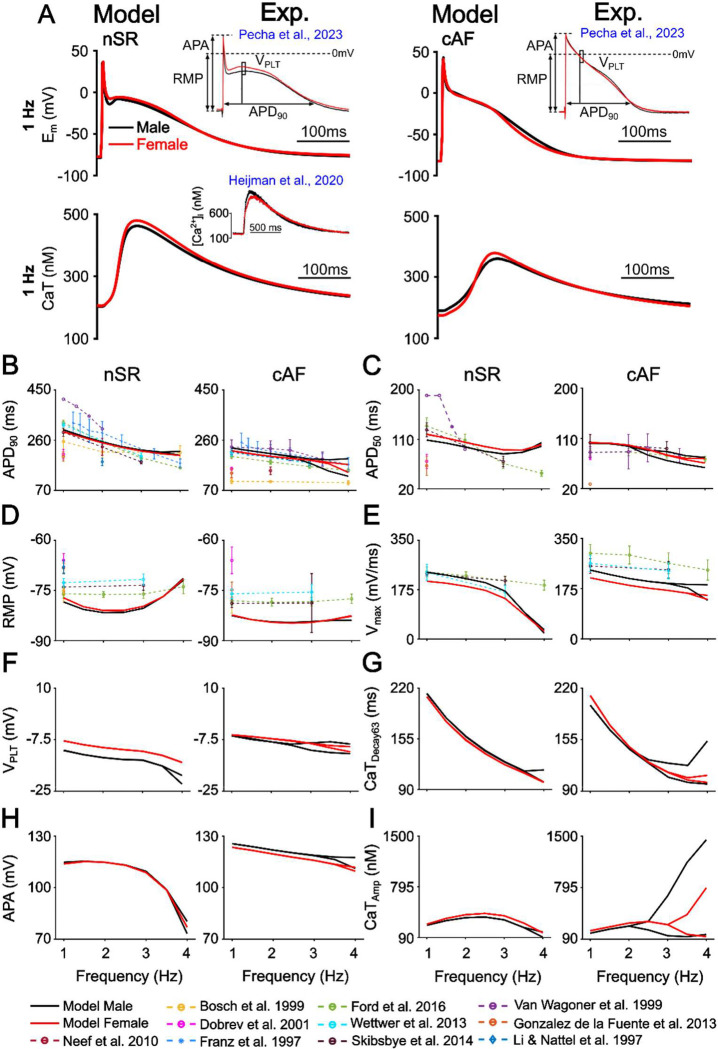
Atrial fibrillation (AF), the most common cardiac arrhythmia, is characterized by notable sex differences in clinical presentation, treatment response, and outcomes. Although prevalence is similar between sexes, women often experience more severe symptoms, higher rates of adverse drug effects, and reduced treatment efficacy. To investigate the underlying sex-specific AF mechanisms, we developed and validated male and female human atrial cardiomyocyte models that integrate known sex-based differences in electrophysiology and calcium (Ca) handling under normal sinus rhythm (nSR) and chronic AF (cAF) conditions. While the model parameterizations were based on limited human data, and the assumptions may not capture the full spectrum of clinical variability, the models reproduced key reported sex-dependent differences in human atrial cardiomyocyte action potential (AP) and Ca transient (CaT) dynamics. Simulations revealed that both sexes exhibited shortened effective refractory periods and wavelengths in cAF vs. nSR. However, females were more prone to delayed afterdepolarizations (DADs), while males were more susceptible to AP duration (APD) and CaT amplitude (CaT) alternans. Population-based modeling identified distinct parameter associations with arrhythmia mechanisms, whereby DAD vulnerability was associated with enhanced ryanodine receptor sensitivity to Ca (in females), and alternans in males correlated with reduced L-type Ca current maximal conductance. Pharmacological simulations revealed sex-specific responses to antiarrhythmic therapies. In males, multiple drug combinations proved effective in restoring APD at 90% repolarization (APD), CaT, and reducing alternans susceptibility, whereas females responded to only one combination improving APD and CaT but with minimal impact on DAD risk. These findings underscore the need for sex-specific therapeutic strategies and support the use of computational modeling in guiding precision medicine approaches against AF.
心房颤动(AF)是最常见的心律失常,其在临床表现、治疗反应和预后方面存在显著的性别差异。尽管男女患病率相似,但女性通常会经历更严重的症状、更高的药物不良反应发生率以及更低的治疗效果。为了研究潜在的性别特异性房颤机制,我们开发并验证了男性和女性人类心房心肌细胞模型,该模型整合了正常窦性心律(nSR)和慢性房颤(cAF)条件下已知的基于性别的电生理和钙(Ca)处理差异。虽然模型参数化基于有限的人类数据,且这些假设可能无法涵盖临床变异性的全貌,但该模型再现了人类心房心肌细胞动作电位(AP)和钙瞬变(CaT)动力学中已报道的关键性别依赖性差异。模拟结果显示,与nSR相比,男女在cAF中均表现出有效不应期和波长缩短。然而,女性更容易发生延迟后去极化(DADs),而男性更容易发生动作电位时程(APD)和钙瞬变幅度(CaT)交替。基于人群的建模确定了与心律失常机制的不同参数关联,其中DAD易感性与ryanodine受体对Ca的敏感性增强(在女性中)相关,而男性中的交替与L型钙电流最大电导降低相关。药理模拟揭示了对抗心律失常治疗的性别特异性反应。在男性中,多种药物组合被证明可有效恢复90%复极化时的APD(APD)、CaT,并降低交替易感性,而女性仅对一种组合有反应,可改善APD和CaT,但对DAD风险影响最小。这些发现强调了针对性别特异性治疗策略的必要性,并支持在指导针对房颤的精准医学方法中使用计算建模。