Shaya Sammy, Uche-Ikonne Okezie, Kilerci Bedirhan, Stevenson Julie, Greystoke Alastair, Cook Natalie, Thistlethwaite Fiona C, Carter Louise, Graham Donna M, Krebs Matthew G
The Christie NHS Foundation Trust, Manchester Academic Health Sciences Centre, Manchester, United Kingdom.
Cancer Research UK Manchester Institute, Manchester, United Kingdom.
J Immunother Precis Oncol. 2025 Aug 25;8(3):222-232. doi: 10.36401/JIPO-25-11. eCollection 2025 Aug.
Patients with advanced solid tumors may be considered for early phase clinical trials investigating the safety, tolerability, and dosing of experimental therapies. Optimizing participant selection is critical to maximize clinical benefit and meet trial endpoints with fewer participants. One in six participants does not meet routine life expectancy requirements (>3 months), highlighting the need for improved prognostication. Variant allele frequency (VAF) in circulating tumor DNA (ctDNA) correlates with overall survival (OS) in advanced solid tumors. We aimed to derive an optimal VAF threshold as a prognostic biomarker to enhance participant selection.
ctDNA testing was performed as part of the TARGET (NIHR Clinical Research Network CPMS ID 39172) and TARGET National (NCT04723316) prospective cohort studies, in patients with advanced solid tumors referred for early phase clinical trials. Maximum (maxVAF) and mean VAF (meanVAF) were compared in their association with OS and ability to delineate favorable and poor outcomes at set threshold points using hazard ratios (HRs). Optimal thresholds of VAF were explored using receiver operating characteristic curve analysis to predict 3-month landmark OS. Univariable and multivariable analysis was performed to determine whether VAF was an independent prognostic marker.
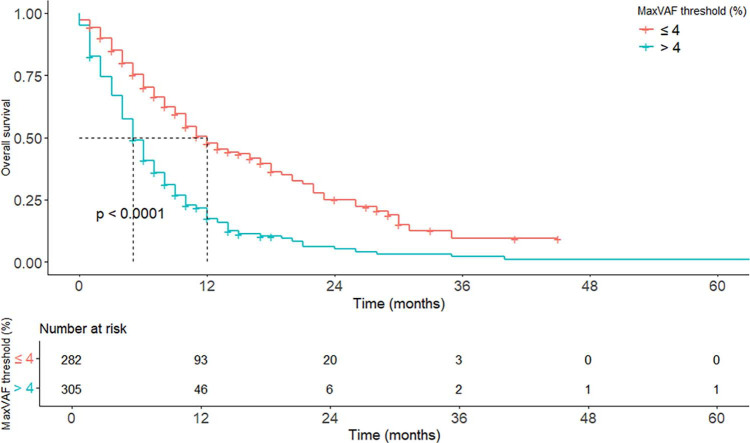
Of 631 patients, 587 had evaluable ctDNA results. MeanVAF and maxVAF exhibited similar correlation with OS (r = -0.32 vs -0.35, respectively) and similar prognostic utility at matched threshold points. A maxVAF value of 4% was selected as optimal for prognostic subgrouping (area under curve 0.77). OS was 5.9 versus 12.1 months ( < 0.0001) for patients with more than 4% and 4% or less maxVAF, respectively. Multivariable analysis confirmed more than 4% maxVAF as independently associated with reduced 3-month landmark OS (HR 2.17 [1.76-2.70], < 0.001).
VAF is an independent prognostic marker in patients with advanced solid tumors, with 4% maxVAF deemed optimal for delineating favorable and poorer prognostic subgroups in this patient cohort. Further validation and integration into existing prognostic scores are warranted.
晚期实体瘤患者可考虑参加早期临床试验,以研究实验性疗法的安全性、耐受性和剂量。优化参与者选择对于最大化临床获益并以更少的参与者达到试验终点至关重要。六分之一的参与者不符合常规预期寿命要求(>3个月),这凸显了改善预后评估的必要性。循环肿瘤DNA(ctDNA)中的变异等位基因频率(VAF)与晚期实体瘤的总生存期(OS)相关。我们旨在得出一个最佳VAF阈值作为预后生物标志物,以优化参与者选择。
ctDNA检测作为TARGET(NIHR临床研究网络CPMS ID 39172)和TARGET National(NCT04723316)前瞻性队列研究的一部分,在转诊至早期临床试验的晚期实体瘤患者中进行。比较最大VAF(maxVAF)和平均VAF(meanVAF)与OS的关联,以及使用风险比(HRs)在设定阈值点区分良好和不良结局的能力。使用受试者工作特征曲线分析探索VAF的最佳阈值,以预测3个月的标志性OS。进行单变量和多变量分析,以确定VAF是否为独立的预后标志物。
631例患者中,587例有可评估的ctDNA结果。MeanVAF和maxVAF与OS表现出相似的相关性(分别为r = -0.32和-0.35),在匹配的阈值点具有相似的预后效用。选择4%的maxVAF值作为预后亚组分析的最佳值(曲线下面积为0.77)。maxVAF大于4%和4%及以下的患者的OS分别为5.9个月和12.1个月(<0.0001)。多变量分析证实,maxVAF大于4%与3个月标志性OS降低独立相关(HR 2.17 [1.76 - 2.70],<0.001)。
VAF是晚期实体瘤患者的独立预后标志物,4%的maxVAF被认为是在该患者队列中区分良好和较差预后亚组的最佳值。有必要进一步验证并将其纳入现有的预后评分中。