Danesh Valerie, Work Brittany D, Chen Denise F, Van Julie, Mart Matthew F, Welch Sarah A, Davidson Mario, Ely E Wesley, Roberson Shawniqua Williams, Jackson James C, Boehm Leanne M
Baylor Scott & White Research Institute, Dallas, Texas.
Baylor College of Medicine, Houston, Texas.
JAMA Netw Open. 2025 Sep 2;8(9):e2531224. doi: 10.1001/jamanetworkopen.2025.31224.
Survivors of critical illness often have ongoing issues that affect functioning, including driving ability.
To examine whether intensive care unit (ICU) delirium is independently associated with long-term changes in driving behaviors.
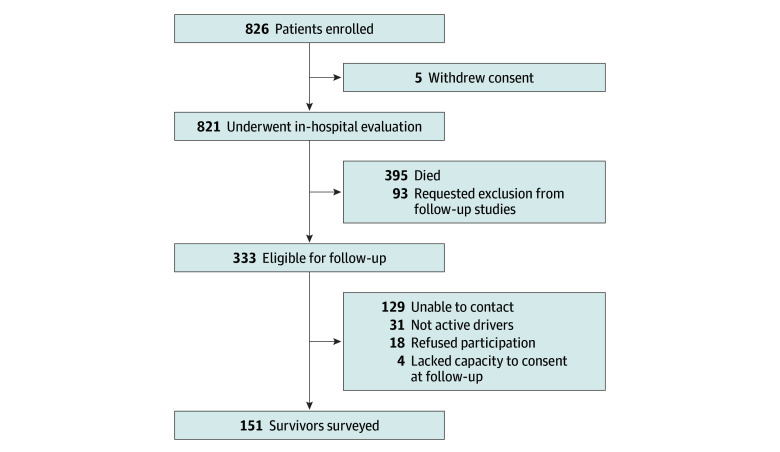
DESIGN, SETTING, AND PARTICIPANTS: This multicenter, longitudinal cohort study included 151 survivors of critical illness residing within 200 miles of Nashville, Tennessee. Survivors were surveyed 2 to 6 years after critical illness to assess the association between delirium duration and driving skills and behaviors (July 1, 2012, to April 30, 2013), and data were analyzed in 2014.
The primary and secondary outcomes were self-rated driving skill (Driver Skill Inventory) and risky driving behaviors (Mini Driver Behavior Questionnaire), respectively. Exploratory outcomes included changes in driving decisions and driving-related attitudes.
Of 333 survivors from the original study, 151 (45.3%) were active drivers and agreed to participation at a median (range) of 3.7 (2.1-6.2) years after critical illness (median [IQR] age at enrollment, 59 [50-64] years; 87 [57.6%] male) with a median (IQR) delirium duration of 1 (0-4) day. Driving resumption occurred at a median (IQR) of 1.9 (0.8-6.0) months after ICU discharge. Delirium duration was not independently associated with self-rated driving skill or risky driving behavior measures (regression coefficients of -0.10 [95% CI, -1.13 to 0.93] for Driver Skill Inventory and-0.46 [95% CI, -1.97 to 1.06] for Mini Driver Behavior Questionnaire). Driving distances after critical illness were significantly lower than prehospitalization estimates (median [IQR], 60 [25-150] vs 105 [58-250] miles per week; P < .001). Driving skill (median [IQR], 34 [26-38] on a 48-point scale; P < .001) and safety orientation measures (median [IQR], 38 [35-46] on a 48-point scale; P < .001) were significantly lower upon return to driving. These decrements persisted among adults 65 years and older.
In this cohort study of survivors of critical illness, ICU delirium was not independently associated with long-term changes in driving behaviors after critical illness; survivors of critical illness self-reported significant decreases in transportation independence and driving skill after hospital discharge, independent of delirium duration during hospitalization. These results suggest that clinicians should consider transportation-related limitations relevant to short- and long-term care planning.
危重症幸存者常常存在影响其功能的持续性问题,包括驾驶能力。
探讨重症监护病房(ICU)谵妄是否与驾驶行为的长期变化独立相关。
设计、背景和参与者:这项多中心纵向队列研究纳入了居住在田纳西州纳什维尔200英里范围内的151名危重症幸存者。在危重症发生2至6年后对幸存者进行调查,以评估谵妄持续时间与驾驶技能和行为之间的关联(2012年7月1日至2013年4月30日),并于2014年对数据进行分析。
主要结局和次要结局分别为自我评定的驾驶技能(驾驶技能量表)和危险驾驶行为(迷你驾驶行为问卷)。探索性结局包括驾驶决策和与驾驶相关态度的变化。
在原研究的333名幸存者中,151名(45.3%)为现职驾驶员,他们同意在危重症发生后的中位时间(范围)3.7(2.1 - 6.2)年参与研究(入组时的中位年龄[四分位间距]为59[50 - 64]岁;87名[57.6%]为男性),谵妄持续时间的中位值(四分位间距)为1(0 - 4)天。恢复驾驶的中位时间(四分位间距)为ICU出院后的1.9(0.8 - 6.0)个月。谵妄持续时间与自我评定的驾驶技能或危险驾驶行为指标无独立相关性(驾驶技能量表的回归系数为 -0.10[95%置信区间,-1.13至0.93],迷你驾驶行为问卷的回归系数为 -0.46[95%置信区间,-1.97至1.06])。危重症后的驾驶里程显著低于住院前的估计值(中位值[四分位间距],每周60[25 - 150]英里对105[58 - 250]英里;P < 0.001)。恢复驾驶时,驾驶技能(48分制的中位值[四分位间距]为34[26 - 38];P < 0.001)和安全意识指标(48分制的中位值[四分位间距]为38[35 - 46];P < 0.001)显著降低。这些下降在65岁及以上的成年人中持续存在。
在这项针对危重症幸存者的队列研究中,ICU谵妄与危重症后驾驶行为的长期变化无独立相关性;危重症幸存者自我报告称出院后交通独立性和驾驶技能显著下降,与住院期间谵妄持续时间无关。这些结果表明,临床医生应考虑与短期和长期护理规划相关的交通方面的限制因素。