Kwon A H, Inui H, Imamura A, Uetsuji S, Kamiyama Y
First Department of Surgery, Kansai Medical University, Osaka, Japan.
Ann Surg. 1998 Mar;227(3):351-6. doi: 10.1097/00000658-199803000-00006.
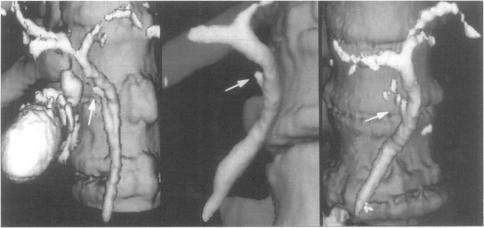
The authors investigated the preoperative feasibility of using spiral computed tomography (SCT) after intravenous infusion cholangiography (IVC-SCT) for laparoscopic cholecystectomy.
In laparoscopic cholecystectomy, the aberrant or unusual anatomy of the bile duct and severe inflammation or adhesions around the gallbladder sometimes require a conversion to open surgery.
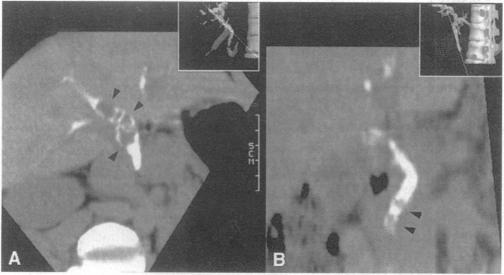
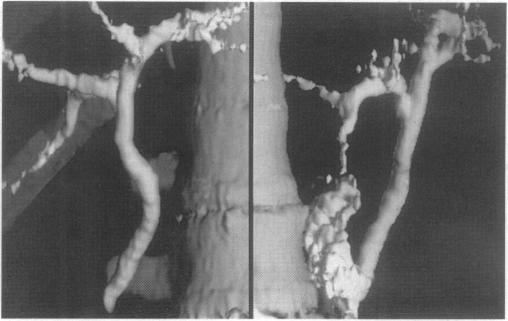
Laparoscopic cholecystectomies (LC's) were attempted on 440 patients, and preoperative IVC-SCT also was attempted in all of these patients. Using this spiral scanning technique, the bile ducts, cystic duct, and gallbladder were assessed for contour abnormalities, relative position, and filling defects. Forty-seven patients were diagnosed with having stones in their common bile duct or common hepatic duct.
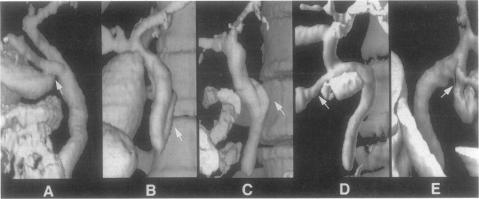
Three-hundred eighty-seven patients out of the 440 patients (88.0%) who were subjected to IVC-SCT had the length and course of their cystic duct successfully determined. Anomalous unions of the cystic duct were seen in 59 (15.2%) of 387 patients with respect to the operative findings, and 48 of 440 patients (10.9%) had severe adhesions to Calot's triangle and the surrounding tissues. In these 48 patients, 45 patients (94%) had a nonvisualized cystic duct on IVC-SCT. The preoperative assessment of the feasibility (dense adhesions obscuring Calot's triangle) of using IVC-SCT demonstrated that the sensitivity, specificity, and accuracy were 93%, 98%, and 94%, respectively. Five patients had to be converted to open surgery, and the overall morbidity rates for patients undergoing laparoscopic cholecystectomy was 0.9% (4 of 440).
The most important factor in assessing the feasibility of using laparoscopic cholecystectomy is not the nonvisualized gallbladder, but the nonvisualized cystic duct on IVC-SCT. IVC-SCT may be of benefit to those patients scheduled to undergo laparoscopic cholecystectomy.
作者研究了静脉输注胆管造影术后行螺旋计算机断层扫描(IVC-SCT)用于腹腔镜胆囊切除术的术前可行性。
在腹腔镜胆囊切除术中,胆管的异常或不寻常解剖结构以及胆囊周围的严重炎症或粘连有时需要转为开腹手术。
对440例患者尝试进行腹腔镜胆囊切除术(LC),所有这些患者也尝试进行术前IVC-SCT。使用这种螺旋扫描技术,评估胆管、胆囊管和胆囊的轮廓异常、相对位置和充盈缺损。47例患者被诊断为胆总管或肝总管有结石。
440例接受IVC-SCT的患者中,387例(88.0%)成功确定了胆囊管的长度和走行。根据手术结果,387例患者中有59例(15.2%)出现胆囊管异常汇合,440例患者中有48例(10.9%)与胆囊三角和周围组织有严重粘连。在这48例患者中,45例(94%)在IVC-SCT上胆囊管未显影。术前对使用IVC-SCT的可行性(致密粘连使胆囊三角模糊不清)进行评估,结果显示敏感性、特异性和准确性分别为93%、98%和94%。5例患者不得不转为开腹手术,接受腹腔镜胆囊切除术患者的总体发病率为0.9%(440例中的4例)。
评估腹腔镜胆囊切除术可行性的最重要因素不是胆囊未显影,而是IVC-SCT上胆囊管未显影。IVC-SCT可能对计划进行腹腔镜胆囊切除术的患者有益。