Jensen R T, Gibril F, Termanini B
Digestive Diseases Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland 20892, USA.
Yale J Biol Med. 1997 Sep-Dec;70(5-6):481-500.
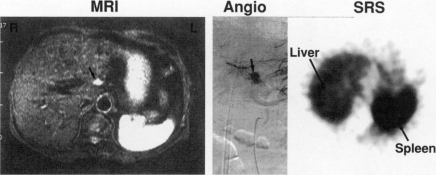
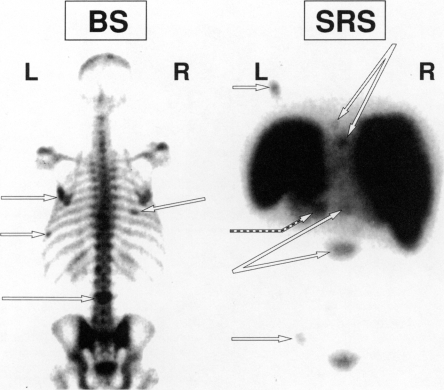
There are six major steps in the management of patients with neuroendocrine tumors (NETs) (carcinoids and pancreatic endocrine tumors). One of the steps that is increasing in its importance is the need to assess primary tumor location and tumor extent in these patients. Without such information, it is not possible to adequately manage these patients. Conventional imaging studies (CT scan, MRI, ultrasound, angiography), functional localization studies measuring hormonal gradients, endoscopic ultrasound, and most recently, somatostatin receptor scintigraphy (SRS) with [125I-DTPA-DPhe1]-octreotide have all been advocated to localize NETs in different studies. Whereas it is now established that for all NETs, except insulinomas, SRS has the greatest sensitivity, it remains unclear whether this increased sensitivity translates into increased clinical usefulness. It, therefore, remains unclear based on fiscal and clinical considerations what should be the recommended algorithm for the use of the different localization methods. To address this issue, we have recently performed two prospective studies on patients with gastrinomas. In this paper, the methods and results of each are summarized and based on these results, an algorithm for localization studies in NETs is proposed. One study assessed the role of SRS in management in 122 patients and shows that the use of SRS changed management in 47 percent of patients according to six different criteria when the patients were stratified according to their principal management problem. Determining whether liver metastases were present is one of the major goals of tumor localization studies and is frequently a source of confusion because of the difficulty in distinguishing small NETs liver metastases from hemangiomas. In the second study, the ability of SRS and other tumor localization methods to distinguish these two possibilities was assessed in 15 patients with small hemangiomas and 15 patients with small hepatic metastases (mean size 1.3 cm). SRS correctly identified 93 percent of the patients with liver metastases and was not positive in any patient with a hemangioma, suggesting it was not a liver metastases. SRS had greater negative and positive predictive value than conventional studies. Based on these two studies, and SRS's greater sensitivity and fiscal considerations, it is proposed that SRS should be the initial tumor imaging study in all NETs except insulinomas, and algorithms for the use of other localization studies in both NETs and insulinomas are proposed.
神经内分泌肿瘤(NETs,包括类癌和胰腺内分泌肿瘤)患者的管理有六个主要步骤。其中一个越来越重要的步骤是需要评估这些患者的原发肿瘤位置和肿瘤范围。没有这些信息,就无法对这些患者进行充分的管理。传统的影像学检查(CT扫描、MRI、超声、血管造影)、测量激素梯度的功能定位研究、内镜超声,以及最近使用[125I-DTPA-DPhe1]-奥曲肽的生长抑素受体闪烁显像(SRS),在不同的研究中都被提倡用于NETs的定位。虽然现在已经确定,对于除胰岛素瘤以外的所有NETs,SRS具有最高的敏感性,但这种增加的敏感性是否转化为更高的临床实用性仍不清楚。因此,基于财政和临床考虑,不同定位方法的推荐使用算法仍不明确。为了解决这个问题,我们最近对胃泌素瘤患者进行了两项前瞻性研究。在本文中,总结了每项研究的方法和结果,并基于这些结果,提出了NETs定位研究的算法。一项研究评估了SRS在122例患者管理中的作用,结果显示,根据六个不同标准,当患者根据其主要管理问题进行分层时,SRS的使用使47%的患者的管理发生了改变。确定是否存在肝转移是肿瘤定位研究的主要目标之一,并且由于难以区分小的NETs肝转移和血管瘤,这常常是一个混淆的来源。在第二项研究中,评估了SRS和其他肿瘤定位方法区分这两种可能性的能力,研究对象为15例患有小血管瘤的患者和15例患有小肝转移瘤的患者(平均大小1.3厘米)。SRS正确识别了93%的肝转移患者,并且在任何血管瘤患者中均未呈阳性,表明不是肝转移。SRS的阴性和阳性预测价值均高于传统研究。基于这两项研究,以及SRS更高的敏感性和财政考虑,建议除胰岛素瘤外,SRS应作为所有NETs的初始肿瘤影像学检查,并提出了NETs和胰岛素瘤中其他定位研究的使用算法。