Gaziev D, Galimberti M, Lucarelli G, Polchi P, Giardini C, Angelucci E, Baronciani D, Sodani P, Erer B, Biagi M D, Andreani M, Agostinelli F, Donati M, Nesci S, Talevi N
Divisione di Ematologia e Centro Trapianti di Midollo Osseo di Muraglia, Azienda Ospedaliera di Pesaro, Pesaro, Italy.
Bone Marrow Transplant. 2000 Apr;25(8):815-21. doi: 10.1038/sj.bmt.1702242.
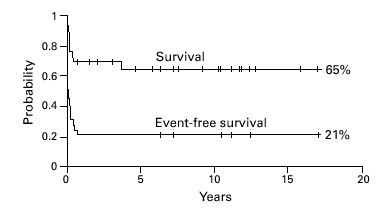
Twenty-nine patients with thalassemia and a median age of 6 years (range 1.1-33 years) were given a BMT from an alternative donor. Six of the 29 donors were HLA-phenotypically identical and two were mismatched relatives, 13 were mismatched siblings and eight were mismatched parents. Six patients received no antigen (relatives), 15 patients one antigen, five patients two antigen and three patients three antigen disparate grafts. Twenty-three patients were in class 2 or class 3, whereas six patients were in class 1. Thirteen patients were given BUCY, nine patients BUCY plus ALG, six patients BUCY plus TBI or TLI and one patient BUCY with prior cytoreductive-immunosuppressive treatment as conditioning. As GVHD prophylaxis four patients received MTX, 22 CsA + MTX + methylprednisolone (MP) and three patients CsA + MP. Thirteen of 29 patients (44.8%) had sustained engraftment. The probability of graft failure or rejection was 55%. There were no significant differences between antigen disparities and graft failure. The incidence of grade II-IV acute GVHD was 47.3% and chronic GVHD was 37.5%. The incidence of acute GVHD was higher in patients receiving one or two antigen disparate in the GVHD direction grafts (vs no antigen) (P EQ 0.04; odds ratio 10.8; 95% CI 1.5-115). The probability of overall and event-free survival was 65% and 21%, respectively, with median follow-up of 7.5 years (range 0.6-17 years) for surviving patients. The degree of HLA disparity between patient and donor did not have a significant effect on survival. The incidence of nonhematologic toxicity was low. Transplant-related mortality was 34%. GVHD (acute or chronic) was a major contributing cause of death (50%) followed by infections (30%). We conclude that at present, due to high graft failure and GVHD rates, BMT from alternative donors should be restricted to patients who have poor life expectancies because they cannot receive adequate conventional treatment or because of alloimmunization to minor blood antigens.
29例地中海贫血患者,中位年龄6岁(范围1.1 - 33岁),接受了来自替代供者的骨髓移植(BMT)。29名供者中,6名HLA表型相同,2名是错配亲属,13名是错配同胞,8名是错配父母。6例患者接受了无抗原(亲属)移植,15例患者接受了1个抗原差异的移植,5例患者接受了2个抗原差异的移植,3例患者接受了3个抗原差异的移植。23例患者处于2级或3级,而6例患者处于1级。13例患者接受了白消安(BUCY)预处理,9例患者接受了BUCY加抗淋巴细胞球蛋白(ALG)预处理,6例患者接受了BUCY加全身照射(TBI)或胸腺照射(TLI)预处理,1例患者接受了BUCY联合先前的细胞减灭性免疫抑制治疗作为预处理。作为移植物抗宿主病(GVHD)预防措施,4例患者接受了甲氨蝶呤(MTX),22例患者接受了环孢素(CsA)+MTX+甲基泼尼松龙(MP),3例患者接受了CsA+MP。29例患者中有13例(44.8%)实现了持续植入。移植物失败或排斥的概率为55%。抗原差异与移植物失败之间无显著差异。II - IV级急性GVHD的发生率为47.3%,慢性GVHD的发生率为37.5%。在GVHD方向上接受1个或2个抗原差异移植的患者(与无抗原移植相比)急性GVHD的发生率更高(P = 0.04;优势比10.8;95%可信区间1.5 - 115)。存活患者的总生存率和无事件生存率分别为65%和21%,中位随访时间为7.5年(范围0.6 - 17年)。患者与供者之间HLA差异程度对生存率无显著影响。非血液学毒性的发生率较低。移植相关死亡率为34%。GVHD(急性或慢性)是主要的死亡原因(50%),其次是感染(30%)。我们得出结论,目前,由于移植物失败和GVHD发生率较高,来自替代供者的BMT应仅限于预期寿命较短的患者,这些患者要么无法接受充分的传统治疗,要么因对次要血型抗原产生同种免疫反应。