Randolph J G
Ann Surg. 1975 May;181(5):586-90. doi: 10.1097/00000658-197505000-00011.
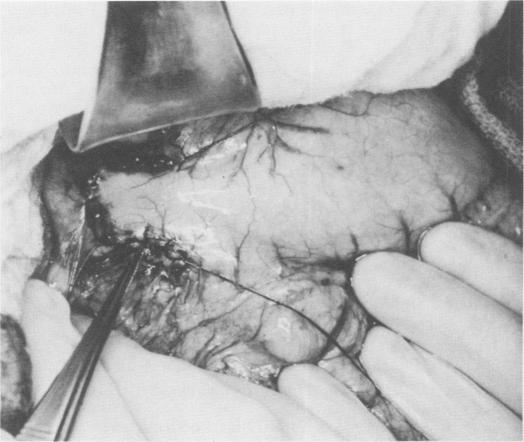
Heineke in 1886 and von Mikulicz in 1887 independently described the popular method of pyloroplasty by longitudinal incision and transverse closure. In some patients, particularly children, the Heineke-Mikulicz procedure has not always been satisfactory because of inadequate size and distortion of the muscular gastroduodenal funnel. In 1958, Moschel and co-workers reintroduced the concept of the Y-V advancement principle to enlarge the pylorus. This operation has not been widely adopted but has a number of attractive features, including simplicity, safety, and maximal channel size with minimal operating time. The standard Y-V principle has been modified in favor of a broadly based U-shaped pedicle constructed from the presenting surface of the gastric antrum which is advanced into an incision made in the anterior duodenum. This operation has been used in 33 patients, who range in age from 3 weeks to 17 years. They have been variously followed from 6 months to 10 years. The surgical need for pyloroplasty in this group of patients included hiatal hernia with delayed gastric emptying (19 patients); vagotomy for ulcer (7 patients); esophageal substitution (4 patients); vagotomy for reflux esophagitis (2 patients); and, in one instance, revision of an obstructed Heineke-Mikulicz pyloroplasty. Complications have been minimal; gastric drainage has been highly satisfactory. In long-term followup, no ill effect has been seen from the presence of antral mucosa in the proximal duodenum.
1886年,海涅克(Heineke)和1887年,冯·米库利奇(von Mikulicz)分别独立描述了通过纵向切口和横向缝合进行幽门成形术的常用方法。在一些患者中,尤其是儿童,由于胃十二指肠漏斗部肌肉尺寸不足和变形,海涅克-米库利奇手术并不总是令人满意。1958年,莫舍尔(Moschel)及其同事重新引入了Y-V推进原则以扩大幽门。该手术尚未被广泛采用,但具有许多吸引人的特点,包括操作简单、安全,能以最短的手术时间获得最大的通道尺寸。标准的Y-V原则已被修改,采用从胃窦部表面构建的宽基底U形蒂,将其推进至十二指肠前部的切口处。该手术已应用于33例患者,年龄从3周至17岁不等。随访时间从6个月至10年不等。这组患者进行幽门成形术的手术适应证包括伴有胃排空延迟的食管裂孔疝(19例);溃疡行迷走神经切断术(7例);食管替代术(4例);反流性食管炎行迷走神经切断术(2例);还有1例是对梗阻性海涅克-米库利奇幽门成形术进行修复。并发症极少;胃引流效果非常令人满意。长期随访显示,十二指肠近端存在胃窦黏膜未见不良影响。