Ballas Samir K
Department of Medicine, Cardeza Foundation for Hematologic Research, Jefferson Medical College, Philadelphia, PA 19107, USA.
Drugs. 2002;62(8):1143-72. doi: 10.2165/00003495-200262080-00003.
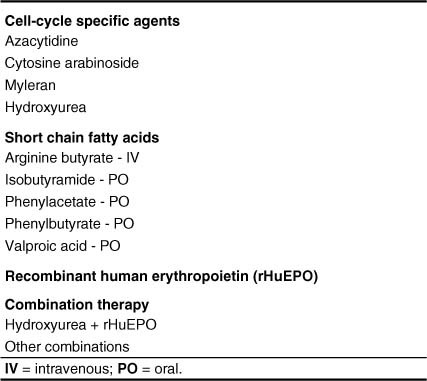
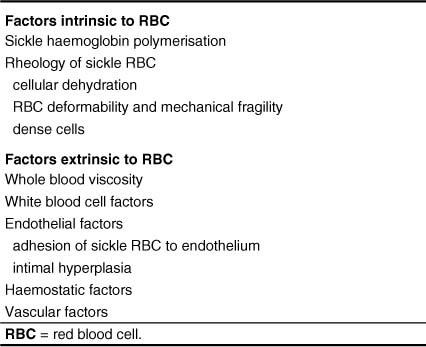
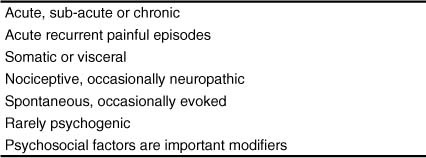
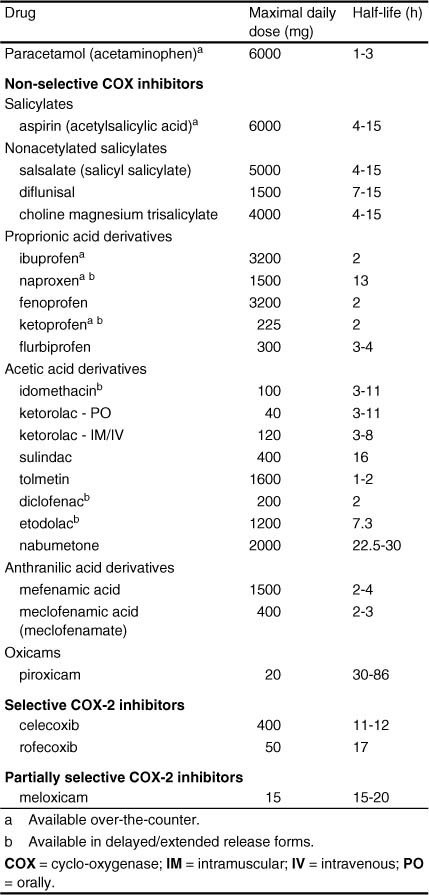
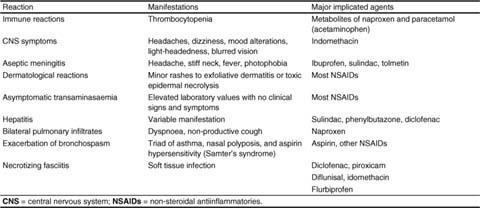
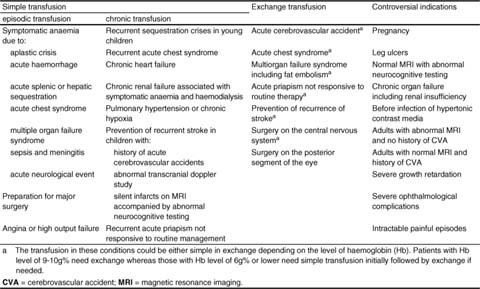
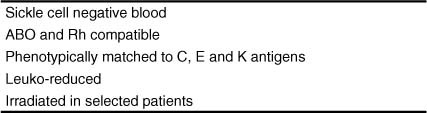
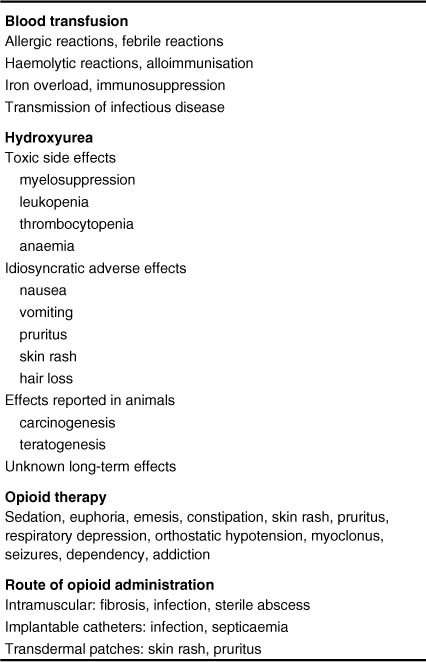
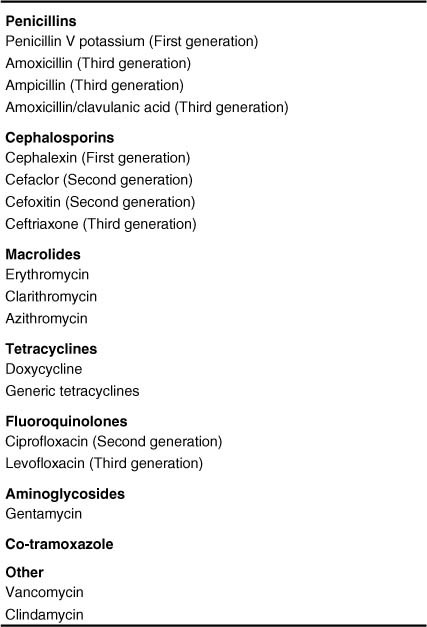
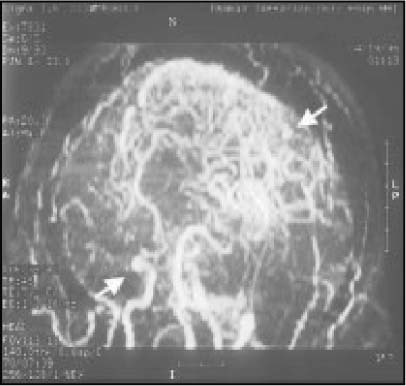
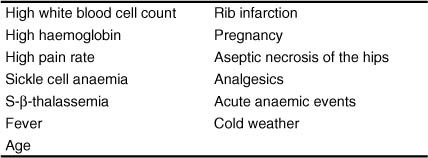
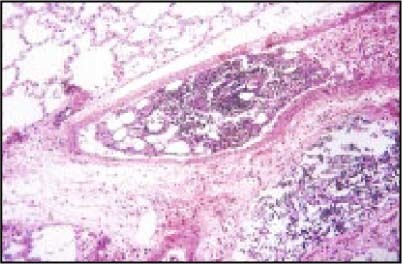
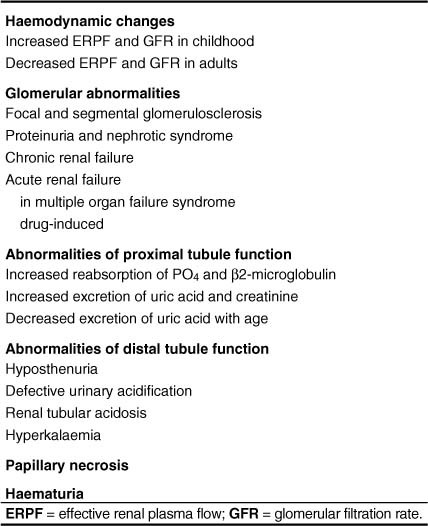
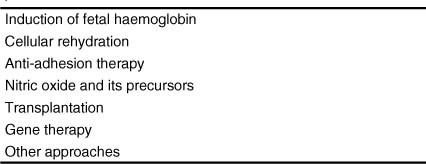
The phenotypic expression of sickle cell anaemia varies greatly among patients and longitudinally in the same patient. It influences all aspects of the life of affected individuals including social interactions, intimate relationships, family relations, peer interactions, education, employment, spirituality and religiosity. The clinical manifestations of sickle cell anaemia are protean and fall into three major categories: anaemia and its sequelae;pain and related issues; andorgan failure including infection. Recent studies on the pathogenesis of sickle cell anaemia have centred on the sequence of events that occur between polymerisation of deoxy haemoglobin (Hb) S and vaso-occlusion. Cellular dehydration, inflammatory response and reperfusion injury seem to be important pathophysiological mechanisms. Management of sickle cell anaemia continues to be primarily palliative in nature, including supportive, symptomatic and preventative approaches to therapy. Empowerment and education are the major aspects of supportive care. Symptomatic management includes pain management, blood transfusion and treatment of organ failure. Pain managment should follow certain priniciples that include assessment, individualisation of therapy and proper utilisation of opioid and nonopioid analgesics in order to acheive adequate pain relief. Blood selected for transfusion should be leuko-reduced and phenotypically matched for the C, E and Kell antigens. Exchange transfusion is indicated in patients who are transfused chronically in order to prevent or delay the onset of iron-overload. Acute chest syndrome is the most common form of organ failure and its management should be agressive, including adequate ventilation, multiple antibacterials and simple or exchange blood transfusion depending on its severity. Preventitive therapy includes prophylactic penicillin in infants and children, blood transfusion (preferably exchange transfusion) in patients with stroke, and hydroxyurea in patients with frequent acute painful episodes. Bone marrow and cord blood transplantation have been successful modalities of curative therapy in selected children with sickle cell anaemia. Newer approaches to preventative therapy include cellular rehydration with agents that inhibit the Gardos channel or the KCl co-transport channel. Curative gene therapy continues to be investigational at the level of the test tube and transgenic mouse models.
镰状细胞贫血的表型表达在患者之间差异很大,并且在同一患者体内随时间也会发生变化。它影响着受影响个体生活的方方面面,包括社会交往、亲密关系、家庭关系、同伴互动、教育、就业、精神信仰和宗教信仰。镰状细胞贫血的临床表现多种多样,主要分为三大类:贫血及其后遗症;疼痛及相关问题;以及包括感染在内的器官衰竭。最近关于镰状细胞贫血发病机制的研究集中在脱氧血红蛋白(Hb)S聚合与血管阻塞之间发生的一系列事件上。细胞脱水、炎症反应和再灌注损伤似乎是重要的病理生理机制。镰状细胞贫血的治疗在本质上仍然主要是姑息性的,包括支持性、对症性和预防性治疗方法。增强患者能力和教育是支持性护理的主要方面。对症治疗包括疼痛管理、输血和器官衰竭的治疗。疼痛管理应遵循某些原则,包括评估、治疗个体化以及合理使用阿片类和非阿片类镇痛药,以实现充分的疼痛缓解。用于输血的血液应进行白细胞去除处理,并在C、E和凯尔抗原表型上匹配。对于长期输血的患者,应进行换血治疗以预防或延迟铁过载的发生。急性胸综合征是最常见的器官衰竭形式,其治疗应积极进行,包括充分通气、使用多种抗菌药物以及根据严重程度进行单纯输血或换血治疗。预防性治疗包括对婴儿和儿童使用预防性青霉素、对中风患者进行输血(最好是换血)以及对频繁发生急性疼痛发作的患者使用羟基脲。骨髓和脐血移植已成为选定的镰状细胞贫血儿童患者治愈性治疗的成功方式。预防性治疗的新方法包括使用抑制加德通道或氯化钾共转运通道的药物进行细胞补液。治愈性基因治疗在试管和转基因小鼠模型层面仍处于研究阶段。