Bachelot T, Gomez F, Biron P, Ray-Coquard I, Soler-Michel P, Philip I, Guastalla J P, Rebattu P, Dumortier A, Droz J P, Blay J Y
Département de Cancérologie Médicale Centre Léon Bérard, 28 rue Laënnec, 69373 Lyon Cedex, France.
Br J Cancer. 2002 Nov 4;87(10):1079-85. doi: 10.1038/sj.bjc.6600631.
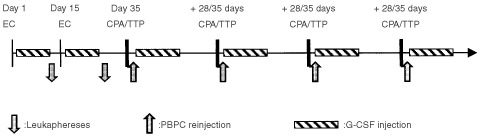
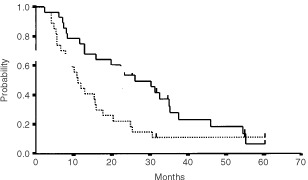
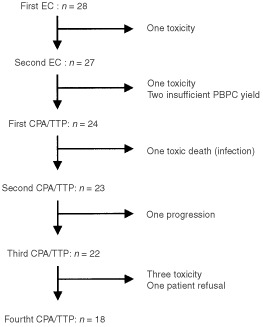
This pilot phase I/II study intended to determine the maximum tolerated dose of cyclophosphamide and thiotepa administered on four consecutive courses with peripheral blood progenitor cell and granulocyte-colony stimulating factor support, as first-line therapy for hormone-refractory metastatic breast cancer patients. Twenty-eight patients were entered in the study. After two courses of epirubicin (120 mg m(-2)) and cyclophosphamide (2 g m(-2)) followed by granulocyte-colony stimulating factor injection and leukaphereses, patients received four cycles of cyclophosphamide and thiotepa. Each cycle was followed by peripheral blood progenitor cell and granulocyte-colony stimulating factor supports, then repeated every 28 to 35 days. Six escalating dose levels of cyclophosphamide and thiotepa were planned, beginning at cyclophosphamide 1.5 g m(-2) and thiotepa 200 mg m(-2). At least three patients were enrolled for each dose level. Eighteen patients completed the study. The maximum tolerated dose was 3000 mg m(-2) cyclophosphamide and 400 mg m(-2) thiotepa per course. Haematological toxicity was manageable on an outpatient basis and did not increase significantly with dose escalation. Dose-limiting toxicity was chemotherapy-induced immunosuppression, which resulted in one toxic death and two life-threatening infections. Median times to treatment failure and survival were 11 and 26 months, respectively. Three patients were alive, free of disease 30 months after completion of the study. Such therapy allows for high-dose intensity and high cumulative doses on a short period of time with manageable toxicity.
这项I/II期先导研究旨在确定在接受外周血祖细胞和粒细胞集落刺激因子支持的情况下,连续四个疗程给予环磷酰胺和塞替派的最大耐受剂量,作为激素难治性转移性乳腺癌患者的一线治疗。28名患者进入该研究。在接受两个疗程的表柔比星(120 mg/m²)和环磷酰胺(2 g/m²)治疗,随后注射粒细胞集落刺激因子并进行白细胞单采后,患者接受四个周期的环磷酰胺和塞替派治疗。每个周期后给予外周血祖细胞和粒细胞集落刺激因子支持,然后每28至35天重复一次。计划了六个递增剂量水平的环磷酰胺和塞替派,起始剂量为环磷酰胺1.5 g/m²和塞替派200 mg/m²。每个剂量水平至少纳入三名患者。18名患者完成了研究。最大耐受剂量为每个疗程环磷酰胺3000 mg/m²和塞替派400 mg/m²。血液学毒性在门诊可控制,且未随剂量递增而显著增加。剂量限制性毒性为化疗诱导的免疫抑制,导致一例毒性死亡和两例危及生命的感染。治疗失败和生存的中位时间分别为11个月和26个月。三名患者在研究完成后30个月仍存活且无疾病。这种治疗方法能够在短时间内实现高剂量强度和高累积剂量,且毒性可控。