Janicki Piotr K, Stoica Cristina, Chapman William C, Wright J Kelly, Walker Garry, Pai Ram, Walia Ann, Pretorius Mias, Pinson C Wright
Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, Tennessee, 37232-4125, USA.
BMC Anesthesiol. 2002 Nov 19;2(1):7. doi: 10.1186/1471-2253-2-7.
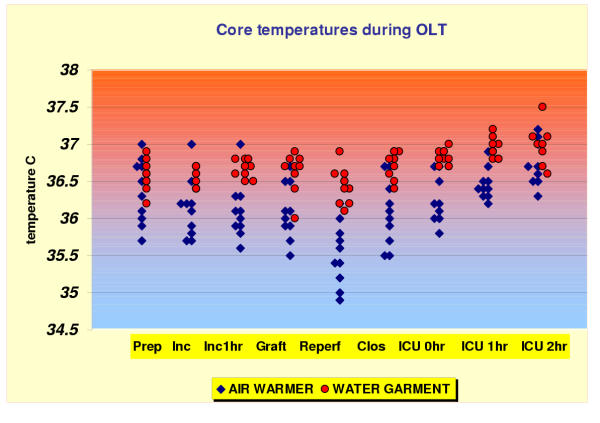
The authors compared two strategies for the maintenance of intraoperative normothermia during orthotopic liver transplantation (OLT): the routine forced-air warming system and the newly developed, whole body water garment. METHODS: In this prospective, randomized and open-labelled study, 24 adult patients were enrolled in one of two intraoperative temperature management groups during OLT. The water-garment group (N = 12) received warming with a body temperature (esophageal) set point of 36.8 degrees C. The forced air-warmer group (N = 12) received routine warming therapy using upper- and lower-body forced-air warming system. Body core temperature (primary outcome) was recorded intraoperatively and during the two hours after surgery in both groups. RESULTS: The mean core temperatures during incision, one hour after incision and during the skin closing were significantly higher (p < 0.05, t test with Bonferroni corrections for the individual tests) in the water warmer group compared to the control group (36.7 PlusMinus; 0.1, 36.7 PlusMinus; 0.2, 36.8 PlusMinus; 0.1 vs 36.1 PlusMinus; 0.4, 36.1 PlusMinus; 0.4, 36.07 PlusMinus; 0.4 degrees C, respectively). Moreover, significantly higher core temperatures were observed in the water warmer group than in the control group during the placement of cold liver allograft (36.75 PlusMinus; 0.17 vs 36.09 PlusMinus; 0.38 degrees C, respectively) and during the allograft reperfusion period (36.3 PlusMinus; 0.26 vs 35.52 PlusMinus; 0.42 degrees C, respectively). In addition, the core temperatures immediately after admission to the SICU (36.75 PlusMinus; 0.13 vs 36.22 PlusMinus; 0.3 degrees C, respectively) and at one hr (36.95 PlusMinus; 0.13 vs 36.46 PlusMinus; 0.2 degrees C, respectively) were significantly higher in the water warmer group, compared to the control group, whereas the core temperature did not differ significantly afte two hours in ICU in both groups. CONCLUSIONS: The investigated water warming system results in better maintenance of intraoperative normothermia than routine air forced warming applied to upper- and lower body.
作者比较了原位肝移植(OLT)术中维持正常体温的两种策略:常规的强制空气加热系统和新开发的全身水衣。方法:在这项前瞻性、随机、开放标签研究中,24例成年患者在OLT术中被纳入两个术中体温管理组之一。水衣组(N = 12)接受体温(食管)设定点为36.8摄氏度的加热。强制空气加热组(N = 12)接受使用上半身和下半身强制空气加热系统的常规加热治疗。术中及术后两小时记录两组患者的体核温度(主要结局)。结果:与对照组相比,水加热组在切口时、切口后一小时及皮肤缝合时的平均核心温度显著更高(p < 0.05,采用Bonferroni校正的t检验进行个体检验)(分别为36.7±0.1、36.7±0.2、36.8±0.1 vs 36.1±0.4、36.1±0.4、36.07±0.4摄氏度)。此外,在植入冷肝移植时(分别为36.75±0.17 vs 36.09±0.38摄氏度)和移植肝再灌注期(分别为36.3±0.26 vs 35.52±0.42摄氏度),水加热组的核心温度显著高于对照组。此外,与对照组相比,水加热组进入外科重症监护病房(SICU)后即刻(分别为36.75±0.13 vs 36.22±0.3摄氏度)和1小时时(分别为36.95±0.13 vs 36.46±0.2摄氏度)的核心温度显著更高,而两组在ICU两小时后的核心温度无显著差异。结论:与应用于上半身和下半身的常规强制空气加热相比,所研究的水加热系统能更好地维持术中正常体温。