Blackwood Kym S, Al-Azem Assaad, Elliott Lawrence J, Hershfield Earl S, Kabani Amin M
National Reference Center for Mycobacteriology, National Microbiology Laboratory, Health, Canada, Winnipeg, MB, Canada.
BMC Infect Dis. 2003 Aug 13;3:18. doi: 10.1186/1471-2334-3-18.
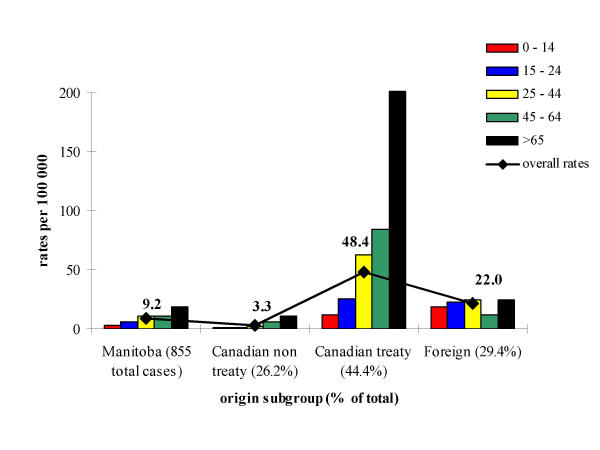
To describe the demographic and geographic distribution of tuberculosis (TB) in Manitoba, thus determining risk factors associated with clustering and higher incidence rates in distinct subpopulations.
Data from the Manitoba TB Registry was compiled to generate a database on 855 patients with tuberculosis and their contacts from 1992-1999. Recovered isolates of M. tuberculosis were typed by IS6110 restriction fragment length polymorphisms. Bivariate and multivariate logistic regression models were used to identify risk factors involved in clustering.
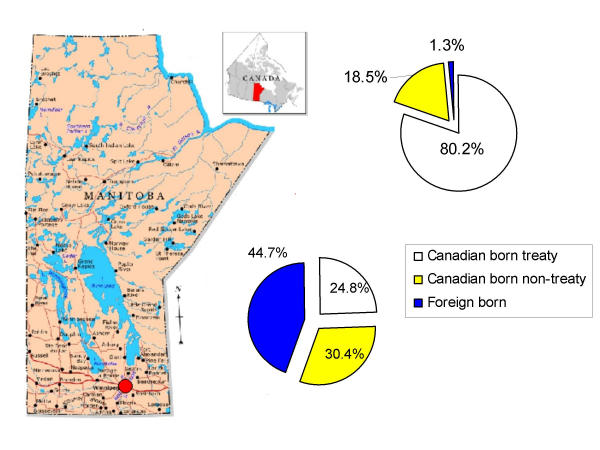
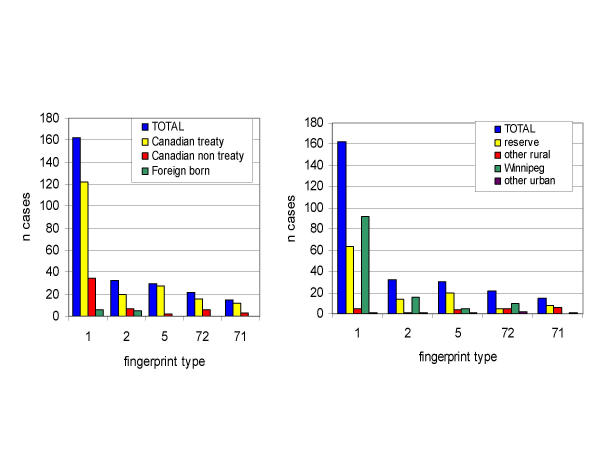
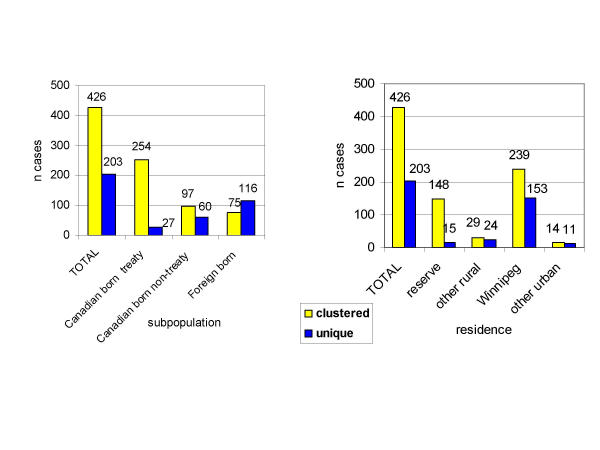
A trend to clustering was observed among the Canadian-born treaty Aboriginal subgroup in contrast to the foreign-born. The dominant type, designated fingerprint type 1, accounts for 25.8% of total cases and 75.3% of treaty Aboriginal cases. Among type 1 patients residing in urban areas, 98.9% lived in Winnipeg. In rural areas, 92.8% lived on Aboriginal reserves. Statistical models revealed that significant risk factors for acquiring clustered tuberculosis are gender, age, ethnic origin and residence. Those at increased risk are: males (p < 0.05); those under age 65 (p < 0.01 for each age subgroup); treaty Aboriginals (p < 0.001), and those living on reserve land (p < 0.001).
Molecular typing of isolates in conjunction with contact tracing data supports the notion of the largest ongoing transmission of a single strain of TB within the treaty-status population of Canada recorded to date. This data demonstrates the necessity of continued surveillance of countries with low prevalence of the disease in order to determine and target high-risk populations for concentrated prevention and control measures.
描述曼尼托巴省结核病(TB)的人口统计学和地理分布,从而确定与不同亚人群中聚集性和较高发病率相关的危险因素。
汇编曼尼托巴省结核病登记处的数据,以生成一个关于1992年至1999年855例结核病患者及其接触者的数据库。通过IS6110限制性片段长度多态性对结核分枝杆菌的回收菌株进行分型。使用双变量和多变量逻辑回归模型来识别聚集相关的危险因素。
与外国出生者相比,在加拿大出生的条约原住民亚组中观察到聚集趋势。主要类型,指定为指纹类型1,占总病例的25.8%和条约原住民病例的75.3%。在居住在城市地区的1型患者中,98.9%居住在温尼伯。在农村地区,92.8%居住在原住民保留地。统计模型显示,获得聚集性结核病的重要危险因素是性别、年龄、种族和居住地。风险增加的人群包括:男性(p < 0.05);65岁以下人群(每个年龄亚组p < 0.01);条约原住民(p < 0.001),以及居住在保留地的人群(p < 0.001)。
分离株的分子分型与接触者追踪数据相结合,支持了迄今为止加拿大条约地位人群中单一菌株结核病最大规模持续传播的观点。这些数据表明,有必要继续监测疾病低流行率国家,以确定高危人群并针对其采取集中的预防和控制措施。