Rosenwald Andreas, Wright George, Leroy Karen, Yu Xin, Gaulard Philippe, Gascoyne Randy D, Chan Wing C, Zhao Tong, Haioun Corinne, Greiner Timothy C, Weisenburger Dennis D, Lynch James C, Vose Julie, Armitage James O, Smeland Erlend B, Kvaloy Stein, Holte Harald, Delabie Jan, Campo Elias, Montserrat Emili, Lopez-Guillermo Armando, Ott German, Muller-Hermelink H Konrad, Connors Joseph M, Braziel Rita, Grogan Thomas M, Fisher Richard I, Miller Thomas P, LeBlanc Michael, Chiorazzi Michael, Zhao Hong, Yang Liming, Powell John, Wilson Wyndham H, Jaffe Elaine S, Simon Richard, Klausner Richard D, Staudt Louis M
Metabolism Branch, National Cancer Institute, National Institute of Health, Bethesda, MD 20892, USA.
J Exp Med. 2003 Sep 15;198(6):851-62. doi: 10.1084/jem.20031074.
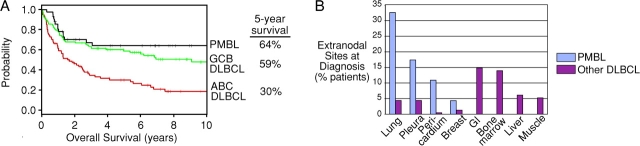
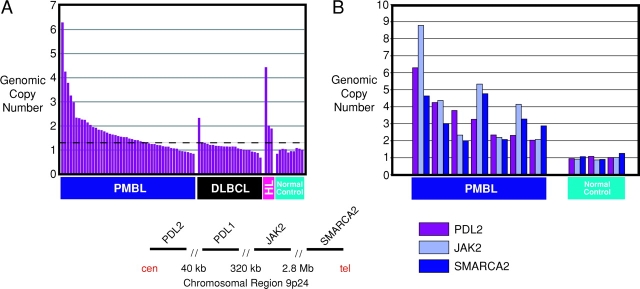
Using current diagnostic criteria, primary mediastinal B cell lymphoma (PMBL) cannot be distinguished from other types of diffuse large B cell lymphoma (DLBCL) reliably. We used gene expression profiling to develop a more precise molecular diagnosis of PMBL. PMBL patients were considerably younger than other DLBCL patients, and their lymphomas frequently involved other thoracic structures but not extrathoracic sites typical of other DLBCLs. PMBL patients had a relatively favorable clinical outcome, with a 5-yr survival rate of 64% compared with 46% for other DLBCL patients. Gene expression profiling strongly supported a relationship between PMBL and Hodgkin lymphoma: over one third of the genes that were more highly expressed in PMBL than in other DLBCLs were also characteristically expressed in Hodgkin lymphoma cells. PDL2, which encodes a regulator of T cell activation, was the gene that best discriminated PMBL from other DLBCLs and was also highly expressed in Hodgkin lymphoma cells. The genomic loci for PDL2 and several neighboring genes were amplified in over half of the PMBLs and in Hodgkin lymphoma cell lines. The molecular diagnosis of PMBL should significantly aid in the development of therapies tailored to this clinically and pathogenetically distinctive subgroup of DLBCL.
使用当前的诊断标准,原发性纵隔B细胞淋巴瘤(PMBL)无法可靠地与其他类型的弥漫性大B细胞淋巴瘤(DLBCL)区分开来。我们使用基因表达谱分析来对PMBL进行更精确的分子诊断。PMBL患者比其他DLBCL患者年轻得多,并且他们的淋巴瘤经常累及其他胸部结构,但不累及其他DLBCL典型的胸外部位。PMBL患者的临床结局相对较好,5年生存率为64%,而其他DLBCL患者为46%。基因表达谱分析有力地支持了PMBL与霍奇金淋巴瘤之间的关系:在PMBL中比在其他DLBCL中表达更高的基因中,超过三分之一在霍奇金淋巴瘤细胞中也有特征性表达。编码T细胞活化调节因子的PDL2是最能将PMBL与其他DLBCL区分开来的基因,并且在霍奇金淋巴瘤细胞中也高度表达。超过一半的PMBL和霍奇金淋巴瘤细胞系中,PDL2和几个相邻基因的基因组位点发生了扩增。PMBL的分子诊断应能显著有助于开发针对DLBCL这一临床和发病机制独特亚组的治疗方法。