Arabi Yaseen, Haddad Samir, Shirawi Nehad, Al Shimemeri Abdullah
Intensive Care Department (MC 1425), King Abdulaziz Medical City, Riyadh, Kingdom of Saudi Arabia.
Crit Care. 2004 Oct;8(5):R347-52. doi: 10.1186/cc2924. Epub 2004 Aug 23.
Despite the integral role played by tracheostomy in the management of trauma patients admitted to intensive care units (ICUs), its timing remains subject to considerable practice variation. The purpose of this study is to examine the impact of early tracheostomy on the duration of mechanical ventilation, ICU length of stay, and outcomes in trauma ICU patients.
The following data were obtained from a prospective ICU database containing information on all trauma patients who received tracheostomy over a 5-year period: demographics, Acute Physiology and Chronic Health Evaluation II score, Simplified Acute Physiology Score II, Glasgow Coma Scale score, Injury Severity Score, type of injuries, ICU and hospital outcomes, ICU and hospital length of stay (LOS), and the type of tracheostomy procedure (percutaneous versus surgical). Tracheostomy was considered early if it was performed by day 7 of mechanical ventilation. We compared the duration of mechanical ventilation, ICU LOS and outcome between early and late tracheostomy patients. Multivariate analysis was performed to assess the impact of tracheostomy timing on ICU stay.
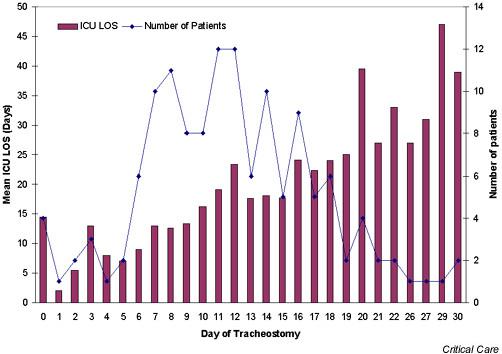
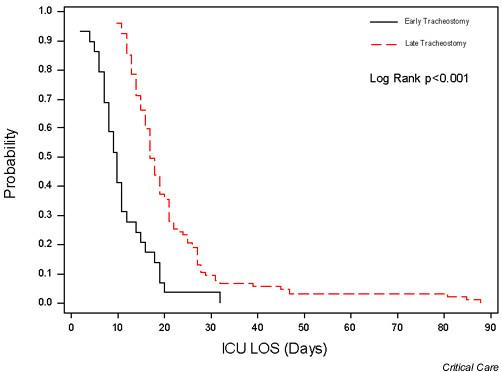
Of 653 trauma ICU patients, 136 (21%) required tracheostomies, 29 of whom were early and 107 were late. Age, sex, Acute Physiology and Chronic Health Evaluation II score, Simplified Acute Physiology Score II and Injury Severity Score were not different between the two groups. Patients with early tracheostomy were more likely to have maxillofacial injuries and to have lower Glasgow Coma Scale score. Duration of mechanical ventilation was significantly shorter with early tracheostomy (mean +/- standard error: 9.6 +/- 1.2 days versus 18.7 +/- 1.3 days; P < 0.0001). Similarly, ICU LOS was significantly shorter (10.9 +/- 1.2 days versus 21.0 +/- 1.3 days; P < 0.0001). Following tracheostomy, patients were discharged from the ICU after comparable periods in both groups (4.9 +/- 1.2 days versus 4.9 +/- 1.1 days; not significant). ICU and hospital mortality rates were similar. Using multivariate analysis, late tracheostomy was an independent predictor of prolonged ICU stay (>14 days).
Early tracheostomy in trauma ICU patients is associated with shorter duration of mechanical ventilation and ICU LOS, without affecting ICU or hospital outcome. Adopting a standardized strategy of early tracheostomy in appropriately selected patients may help in reducing unnecessary resource utilization.
尽管气管切开术在重症监护病房(ICU)收治的创伤患者管理中发挥着不可或缺的作用,但其实施时机仍存在很大的实践差异。本研究的目的是探讨早期气管切开术对创伤ICU患者机械通气时间、ICU住院时间及预后的影响。
从一个前瞻性ICU数据库中获取以下数据,该数据库包含了5年间所有接受气管切开术的创伤患者的信息:人口统计学资料、急性生理与慢性健康状况评估II评分、简化急性生理评分II、格拉斯哥昏迷量表评分、损伤严重程度评分、损伤类型、ICU及医院预后、ICU及医院住院时间(LOS)以及气管切开术的类型(经皮与手术)。如果在机械通气第7天之前进行气管切开术,则视为早期气管切开术。我们比较了早期和晚期气管切开术患者的机械通气时间、ICU住院时间及预后。进行多变量分析以评估气管切开术时机对ICU住院时间的影响。
在653例创伤ICU患者中,136例(21%)需要进行气管切开术,其中29例为早期气管切开术,107例为晚期气管切开术。两组患者的年龄、性别、急性生理与慢性健康状况评估II评分、简化急性生理评分II及损伤严重程度评分无差异。早期气管切开术患者更易发生颌面损伤且格拉斯哥昏迷量表评分较低。早期气管切开术患者的机械通气时间显著缩短(均值±标准误:9.6±1.2天对18.7±1.3天;P<0.0001)。同样,ICU住院时间也显著缩短(10.9±1.2天对21.0±1.3天;P<0.0001)。气管切开术后,两组患者从ICU出院的时间相当(4.9±1.2天对4.9±1.1天;无显著差异)。ICU及医院死亡率相似。通过多变量分析,晚期气管切开术是ICU住院时间延长(>14天)的独立预测因素。
创伤ICU患者早期气管切开术与机械通气时间及ICU住院时间缩短相关,且不影响ICU或医院预后。在适当选择的患者中采用标准化的早期气管切开术策略可能有助于减少不必要的资源利用。